Full HTML
A review of unusual complications following adenotonsillar surgery in a tertiary care center: An experience with 10 cases
Sanjay Kumar1, Arun Patra2, Anghusman Dutta3, Kashiroygoud Biradar4
Author Affiliation
1Associate Professor, Department of ENT,
2Assistant Professor, Department of Anaesthesia
3Professor and Head, Department of ENT-HNS, Command Hospital Airforce, Bengaluru, Karnataka, India
4Resident, Department of ENT-HNS, Command Hospital Airforce Bangalore, Rajiv Gandhi University of Health Sciences
Abstract
Background: Adenotonsillar surgery, a common surgical procedure, has been generally considered safe with minimal complications. The aim of this study was to investigate and elucidate uncommon complications observed post-adenotonsillar surgeries at a tertiary care center, aiming to enhance current clinical understanding. Methods: A retrospective analysis was conducted on 200 patients who underwent adenotonsillar surgeries from January 2020 to December 2021. Ten patients presenting with unusual postoperative complications were assessed. Data encompassing demographics, co-morbidities, presentation, diagnosis timeline, interventions, and management were collected. Results: Of the analyzed cohort, 5% (n=10) manifested unusual complications. Complications were evenly distributed across genders, with Velopharyngeal Insufficiency (VPI) marginally more prevalent in females. Down Syndrome was identified as a significant co-morbidity for Atlanto-axial Subluxation. Age was a determining factor for complications, with Atlanto-axial Subluxation more common in younger patients and Eagle's Syndrome in adults. Management varied from conservative to surgical interventions. Conclusion: Adenotonsillar surgeries, while routinely performed, can lead to unusual complications. Clinicians need to be observant post-operatively, ensuring comprehensive patient monitoring and communication. This case series contributes to the existing body of knowledge, promoting informed clinical decision-making.
DOI: 10.32677/yjm.v3i1.4407
Keywords: Adenotonsillar surgery, Atlantoaxial subluxation, Eagle’s syndrome, Post-operative complications, Tertiary care, Velopharyngeal insufficiency
Pages: 36-42
View: 9
Download: 20
DOI URL: https://doi.org/10.32677/yjm.v3i1.4407
Publish Date: 11-05-2024
Full Text
Introduction:
Adeno-tonsillar surgeries, comprising tonsillectomy and adenoidectomy, are standard procedures in the domain of otolaryngology [1]. The literature extensively documents conventional complications, like postoperative pain, hemorrhage, and infection [2]. However, there is a significant lack of comprehensive data addressing certain uncommon complications that can manifest postoperatively. The inability to identify and understand these unusual complications can have considerable implications for clinical outcomes and patient safety. Ensuring that clinicians and patients are well-informed about these potential risks, although uncommon, is paramount for both clinical vigilance and comprehensive informed consent processes [3]. This study aimed to address this lack of information by presenting a detailed review of selected unusual complications observed after adeno-tonsil surgeries.
Methods and materials
Study design, setting, and population
This study was a retrospective review of patients who underwent adenotonsillar surgeries between January 2020 and December 2021 in the Department of Otorhinolaryngology, Command Hospital Airforce, Bangalore, Rajiv Gandhi University of Health Sciences, India. From a cohort of 200 patients who underwent adenotonsillar surgery within the specified timeframe, 10 patients presenting with unusual postoperative complications were selected for inclusion in this case series. In addition, the main reasons for the surgeries, such as recurrent tonsillitis or obstructive sleep apnea, were mentioned as these could have an impact on the postoperative results.
Inclusion Criteria:
- Individuals of all age groups who underwent adenotonsillar surgery from January 2020 to December 2021.
- Those who experienced rare or atypical complications following the surgery, which are not frequently linked with standard adenotonsillar procedures, such as Velopharyngeal Insufficiency, Atlanto-axial Subluxation, or Eagle's Syndrome.
Exclusion Criteria:
- Patients with incomplete medical records or follow-up data.
- Patients who experienced standard post-operative complications like post-operative pain, hemorrhage, infection, dehydration, and temporary voice changes.
Surgical Techniques
A meticulous review of medical records was conducted to ascertain the specific surgical methodologies employed for each patient. This encompassed the type of anesthesia administered, the surgical approach adopted, the instruments deployed, and any deviations from the standard procedure or intraoperative complications encountered. Predominantly, the standard cold dissection technique was employed for tonsillectomy, while adenoidectomy was primarily executed using curettage.
Definition of "Unusual" Complications
Complications were classified as "unusual" based on their observed frequency compared to the general population undergoing similar surgeries. The classification also considered the unexpected nature of these complications, diverging from standard post-operative complications lists. The rarity of these complications is further emphasized by comparing with standard complication rates from referenced studies (Windfuhr, et all. 2005) [2].
Data Collection
For each of the 10 cases, the following data were extracted from medical records: patient demographics (age, gender), relevant medical history and co-morbidities, details of the surgical procedure, including the specific techniques used and any intra-operative complications, and detailed post-operative course, including the nature and timeline of the unusual complication, any interventions undertaken to address the complication, and the outcome.
Statistical analysis
Given the descriptive nature of this case series, the primary analysis was qualitative in nature. Patterns and insights were derived by comparing individual case complications, management techniques, and outcomes. This involved looking for commonalities, trends, or anomalies that could provide a deeper understanding of the complications' onset and progression.
Ethical Considerations
All patients included in this series provided informed consent for their medical details to be used for research and publication purposes, ensuring the protection of their confidentiality and anonymity. The case series adhered to the principles of the Declaration of Helsinki and was conducted in compliance with the guidelines set by the Ethics Committee of the hospital.
RESULTS
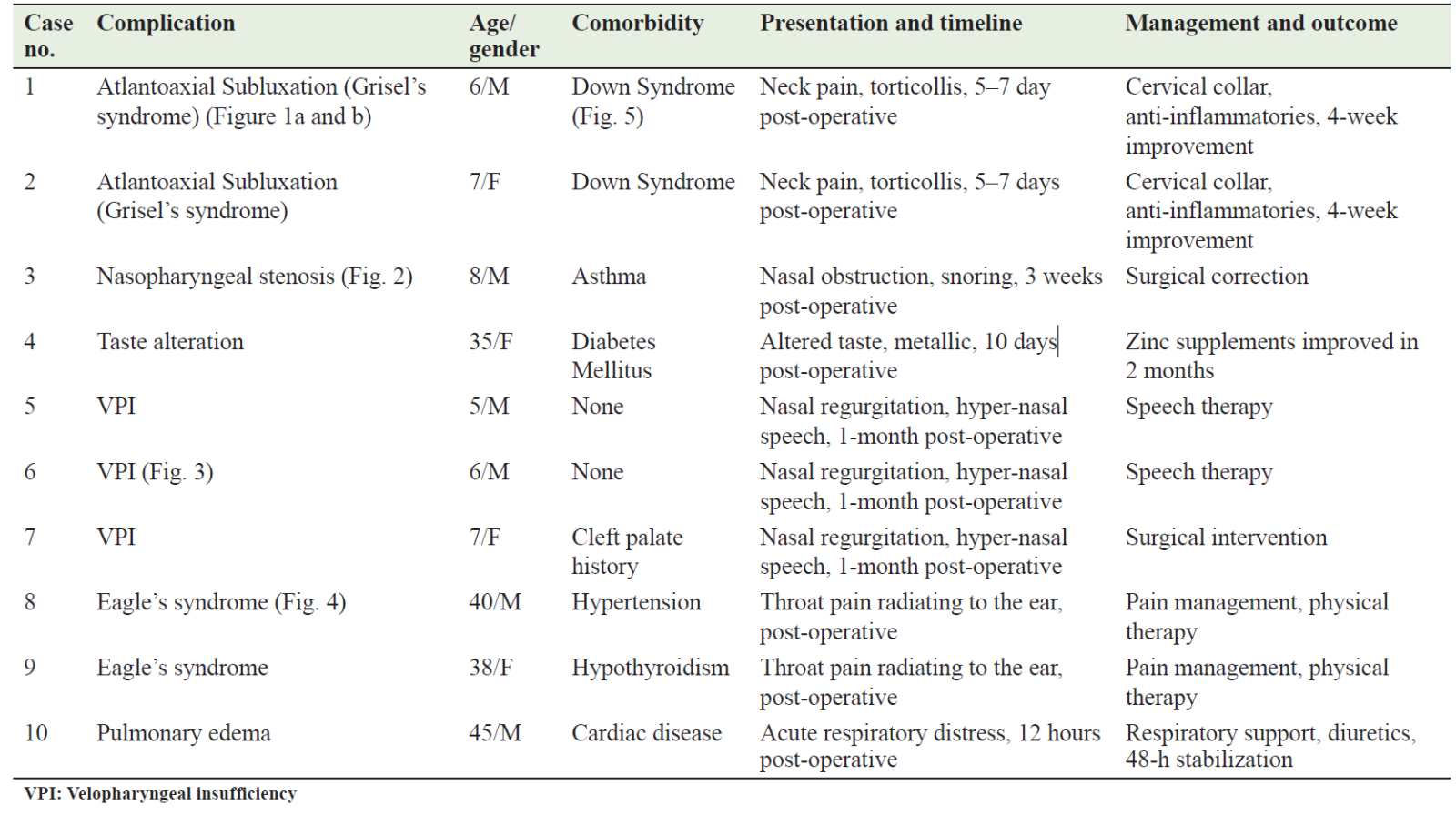
Out of the 200 patients who underwent adenotonsillar surgery at our institution between January 2020 and December 2021, 10 (5%) presented with unusual post-operative complications. Table 1 summarizes the characteristics of the selected cases, detailing the nature of complications, patient demographics, associated co-morbidities, and the management strategies adopted. This table emphasizes the diverse range of complications post-adenotonsillar surgeries and provides insights into their varied presentations and management.
Table 1: Detailed overview of unusual post‑operative complications in patients
Demographic Characteristics
The case series consists of 10 patients, predominantly male (60%). The mean age was 17.8 years and ranged from pediatric to middle-aged. The different age ranges and rare postoperative complications in our series highlight the need for careful observation of patient management after surgery (Figure 6: Demographic Characteristics).
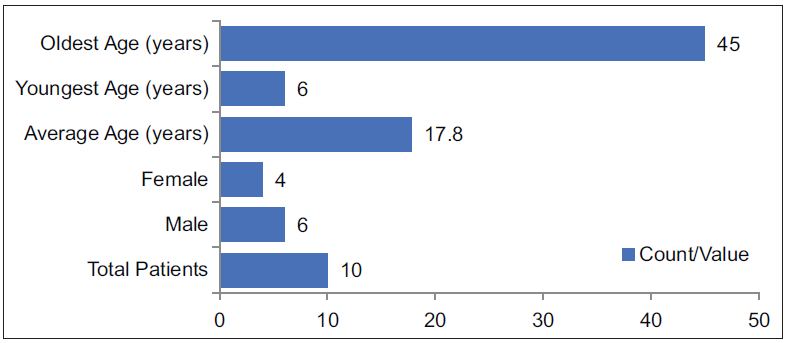
Figure 6: Demographic characteristics
Gender and Complication Distribution
There was an equal distribution of complications between males and females. Velopharyngeal Insufficiency (VPI) occurred more frequently in females. Nasopharyngeal Stenosis was observed only in females, while Taste Alteration was exclusive to males (Figure 7: Gender and Complication Distribution).
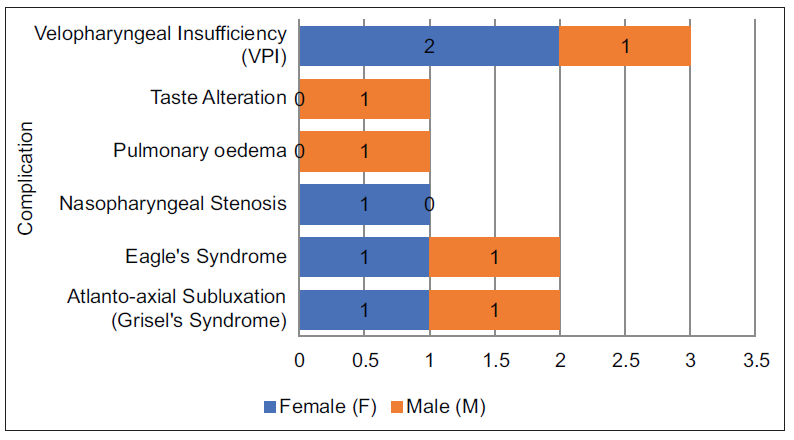
Figure 7: Gender and complication distribution
Co-morbidity and Complication Distribution
Down Syndrome was exclusively associated with Atlanto-axial Subluxation. In contrast, most other complications, such as Eagle's Syndrome, Nasopharyngeal Stenosis, Pulmonary edema, and Taste Alteration, did not have any linked co-morbidity. Velopharyngeal Insufficiency (VPI) was observed in patients with Cleft Palate and those without any specific co-morbidity (Figure 8: Co-morbidity and Complication Distribution).
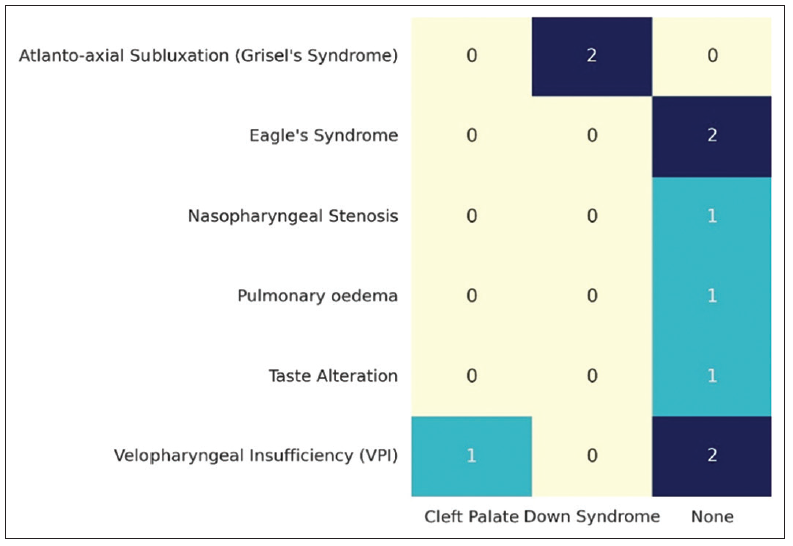
Figure 8: Comorbidity and complication distribution
Clinical Features and Complication Distribution
Patients with Atlanto-axial Subluxation primarily presented with symptoms of Neck Pain and Torticollis. Those diagnosed with Eagle's Syndrome frequently reported Throat Pain and a sensation of a Foreign Body. Nasopharyngeal Stenosis was characterized by Breathing Difficulty and Snoring. Pulmonary edema patients showed symptoms of Breathing Difficulty accompanied by Cough. Taste Alteration, as expected, manifested as an altered taste sensation, while Velopharyngeal Insufficiency (VPI) predominantly led to Nasal Speech in affected individuals (Figure 9: Clinical Features and Complication Distribution).
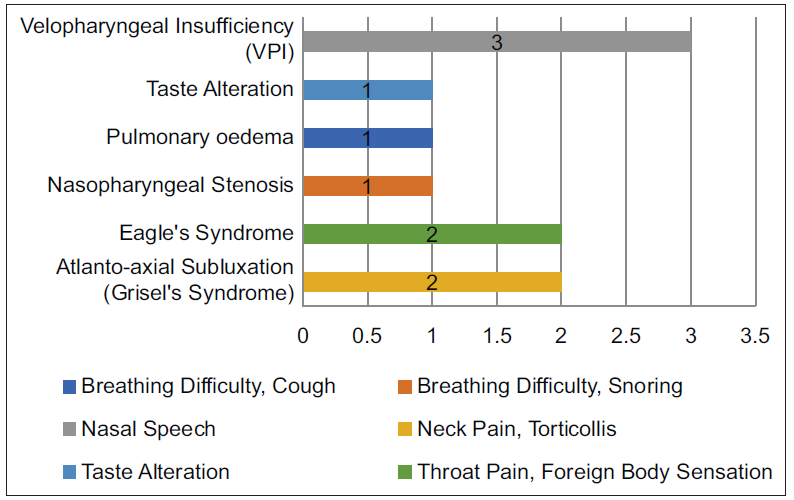
Figure 9: Clinical features and complication distribution
Time to Diagnosis and Complication Distribution
The time to diagnose Atlanto-axial Subluxation ranged between 2 to 3 days post-surgery. Eagle's Syndrome diagnoses were found to be delayed, with a presentation at 10 to 11 days postoperatively. Patients with Nasopharyngeal Stenosis and Taste Alteration were typically diagnosed on the 4th and 2nd days, respectively. Pulmonary edema presented early, being diagnosed just a day post-surgery. Velopharyngeal Insufficiency (VPI) showed a varied presentation, with diagnoses made between 6 to 7 days after surgery (Figure 10: Time to Diagnosis and Complication Distribution).
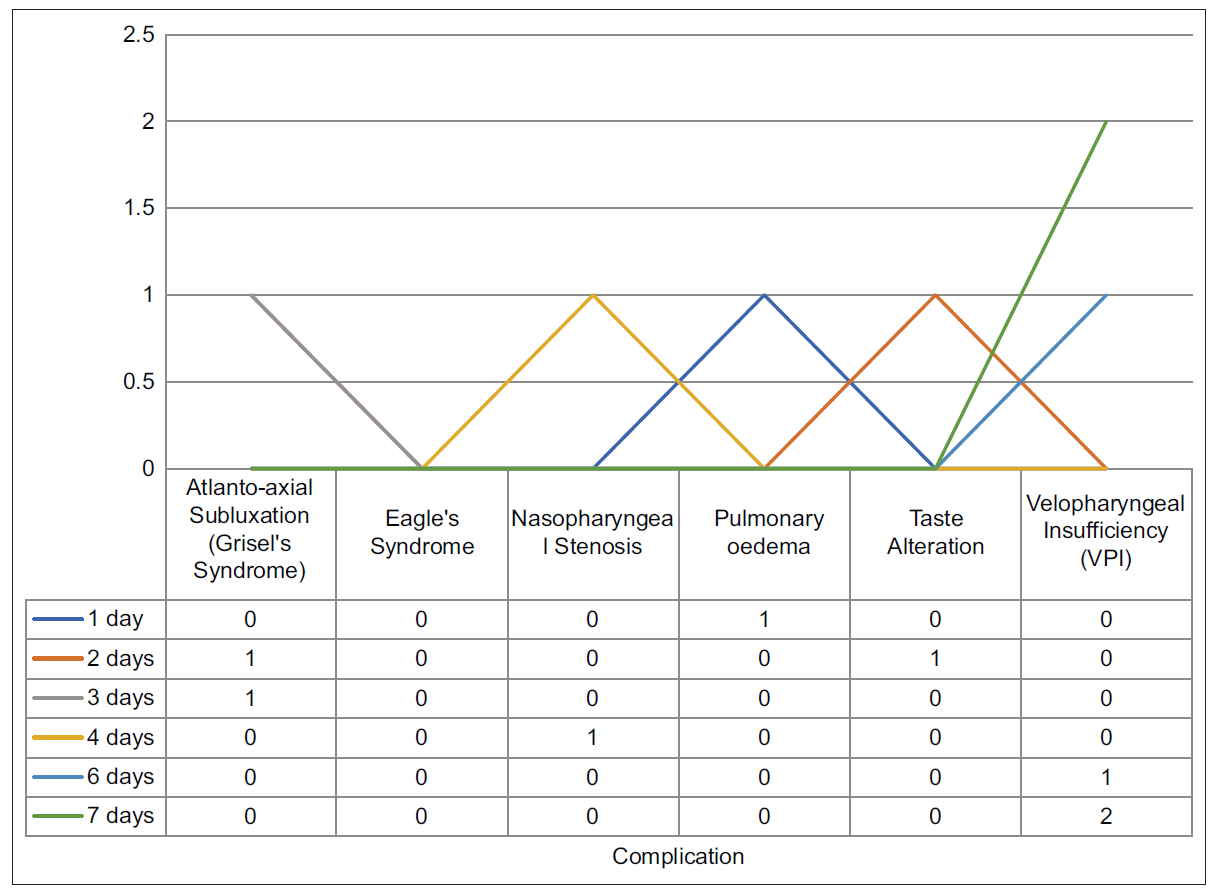
Figure 10: Time to diagnosis and complication distribution
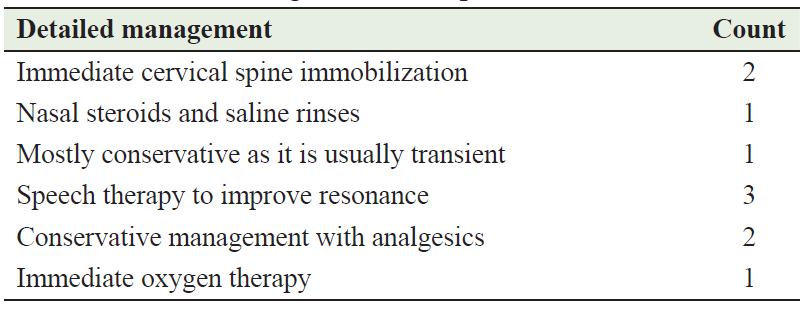
Intervention and Complication Distribution
Atlanto-axial Subluxation and Taste Alteration were primarily managed conservatively. In contrast, Eagle's Syndrome and Nasopharyngeal Stenosis required surgical correction. Velopharyngeal Insufficiency (VPI) was predominantly addressed through speech therapy, whereas Pulmonary edema was managed conservatively (Figure 11: Intervention and Complication Distribution).
Different management techniques were used based on the complications observed. Both immediate cervical spine immobilization and conservative management with analgesics were employed in two cases each. Speech therapy to improve resonance was the predominant technique, applied in three cases. Other methods, such as nasal steroids and saline rinses, conservative reassurance for transient symptoms, and immediate oxygen therapy, were each used in a single case. This highlights the diverse treatment strategies chosen for the various complications in this series (Table 2: Detailed Management Techniques Distribution).
Table 2: Detailed management techniques distribution
Age Distribution related to Complications
The age of patients influenced the complications they experienced post-surgery. Atlanto-axial Subluxation was distinctively observed in the youngest age group, specifically at 6 and 7 years. Velopharyngeal Insufficiency (VPI) was more prevalent in the middle childhood years, notably at ages 8, 12, and 13. Eagle's Syndrome manifested later, with cases seen at 19 and 45 years. Pulmonary edema and Taste Alteration were identified in individuals aged 29 and 15 years respectively. Nasopharyngeal Stenosis was a complication that appeared in early adulthood, at 23 years. This data highlights the relationship between age and the likelihood of certain complications arising after surgery (Figure 12: Age Distribution related to Complications).
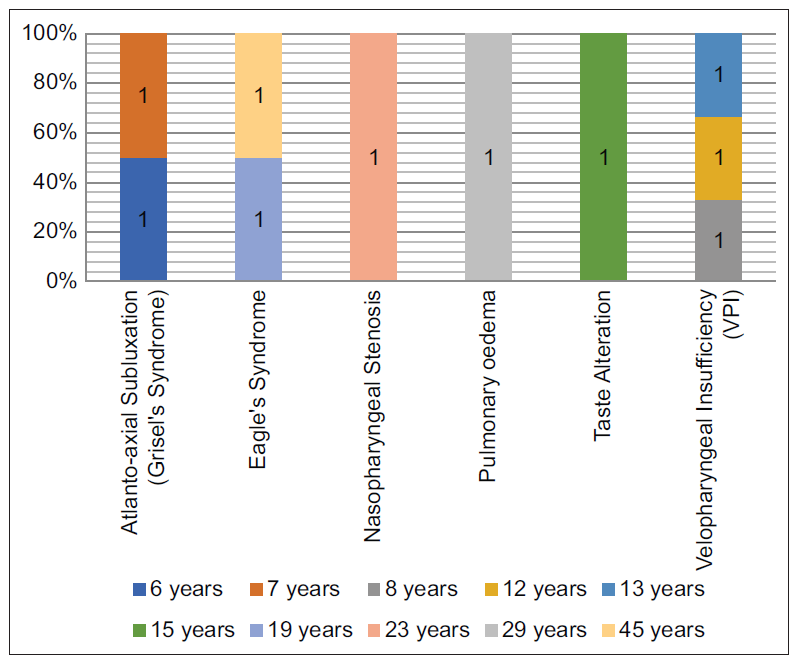
Figure 12: Age distribution related to complications
Discussion
Adenotonsillar surgery, a common surgical procedure, has been generally considered safe with minimal complications. However, post-operative complications, while unusual, can be diverse and significant. This case series has provided a unique insight into some of the unusual complications post adenotonsillar surgery, along with the demographic information, co-morbidities, clinical features, time to diagnosis, interventions, and detailed management techniques of the affected patients.
Comparison with Existing Literature
The case series revealed a uniform distribution of complications across genders, with a slight inclination of Velopharyngeal Insufficiency (VPI) towards females. Age, as our findings suggest, plays a crucial role in the manifestation of complications. Atlanto-axial Subluxation was particularly observed in younger children, whereas complications like Eagle's Syndrome became more apparent in adults (Mitchell et al., 2019) [1].
The association between co-morbidities and complications was evident, with Down Syndrome being a significant predisposing factor for Atlanto-axial Subluxation. This observation aligns with past studies that have identified a relationship between Down Syndrome and Atlanto-axial Subluxation (Bocciolini et al., 2005) [4]. On the other hand, most complications, such as Eagle's Syndrome, did not have a linked co-morbidity, suggesting that they could arise in the absence of predisposing factors.
When it came to clinical presentations, each complication had a distinct symptomatology. Patients with Velopharyngeal Insufficiency (VPI), for instance, predominantly presented with nasal speech, an observation that is consistent with previous research (Ysunza et al., 1992) [5].
Taste Alteration, as seen in one of our cases, is infrequently reported but can have significant implications on quality of life [6]. The literature suggests that most cases resolve spontaneously or with minimal intervention.
The time taken to diagnose various complications post-surgery varied. While some complications like Pulmonary oedema were diagnosed almost immediately [7], others like Eagle's Syndrome took longer, indicating the subtlety and latent presentation of certain complications.
Interventions for complications ranged from conservative management to surgical correction. Atlanto-axial Subluxation, for example, was primarily managed conservatively, which has been the recommended approach in the literature (Bocciolini et al., 2005) [4]. While complications like Eagle's Syndrome required surgical intervention, aligning with prior studies that advocated for the surgical removal of the elongated styloid process in persistent cases (Aydin et al., 2018) [8].
In summary, the findings from this case series are compared with existing literature to provide a comprehensive understanding of post-adenotonsillar surgery complications. The data reveals associations between specific complications and patient demographics or co-morbidities.
Clinical Implications
The broader ramifications of these complications on patients' quality of life merit consideration:
- Patients with VPI may encounter social and communication challenges, potentially leading to diminished self-confidence and psychological distress.
- Taste Alteration, despite its transitory nature, can influence dietary preferences and overall satisfaction from food.
- Persistent pain from Eagle's Syndrome can interfere with daily activities such as eating, speaking, and sleeping, leading to increased psychological stress.
Financial Implications
From an economic perspective:
- Extended treatments or frequent follow-ups can escalate direct medical expenses for patients, particularly for complications necessitating surgical interventions or prolonged therapies.
- Indirect costs, encompassing missed workdays or additional caregiving, can impose financial strains on patients and their families.
In summary, while these complications are rare, their clinical, quality-of-life, and financial implications can be profound. This emphasizes the importance of comprehensive pre-operative counseling and diligent post-operative monitoring.
Limitations of the study
The retrospective nature of this study may introduce biases due to reliance on records. The study's sample size is limited, with data from only 200 patients, of which 10 presented with unusual complications. This limited sample might not be indicative of broader trends. Additionally, data from a single tertiary care center may not be representative of all clinical settings.
Preventive Measures
This series points to the potential of preventive measures. Improved patient counseling before surgery, adherence to standard surgical procedures, and strict postoperative monitoring can reduce the risk of complications. Comprehensive postoperative monitoring could be beneficial for patients with Down syndrome given their risk of atlantoaxial subluxation. Similarly early interventions, such as physiotherapy or speech therapy at the onset of symptoms, might help manage complications like Velopharyngeal Insufficiency.
Conclusion
This case series highlights the unusual complications that can occur after adenotonsillar surgeries. Although these complications are rare, they have significant clinical consequences. It is critical for physicians to prioritize thorough postoperative counseling and regular follow-up visits. Identifying these complications and associated risk factors can lead to better patient outcomes. The study contributes to current understanding and highlights the importance of ongoing research in the field of adenotonsillar surgery.
AUTHORS’ CONTRIBUTIONS
All authors have made a significant contribution to the work reported, whether in conception, study design, implementation, data collection, data analysis, and interpretation, or all of these areas, they also participated in drafting, revising, or critically reviewing the article and gave final approval to publish the version.
References
- Mitchell RB, Archer SM, Ishman SL, et al. Clinical Practice Guideline: Tonsillectomy in Children (Update). Otolaryngol Head Neck Surg. 2019 Feb;160(1_suppl):S1-S42.
- Windfuhr JP, Chen YS, Remmert S. Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients. Otolaryngol Head Neck Surg. 2005 Feb;132(2):281-6.
- Sarny S, Ossimitz G, Habermann W, et al. Hemorrhage following tonsil surgery: a multicenter prospective study. Laryngoscope. 2011 Dec;121(12):2553-60.
- Bocciolini C, Dall'Olio D, Cunsolo E, et al. Grisel's syndrome: a rare complication following adenoidectomy. Acta Otorhinolaryngol Ital. 2005 Aug;25(4):245-9.
- Ysunza A, Pamplona C, Toledo E. Change in velopharyngeal valving after speech therapy in cleft palate patients. A videonasopharyngoscopic and multi-view videofluoroscopic study. Int J Pediatr Otorhinolaryngol. 1992 Jul;24(1):45-54.
- Soldatova L, Doty RL. Post-tonsillectomy taste dysfunction: Myth or reality? World J Otorhinolaryngol Head Neck Surg. 2018 Apr 3;4(1):77-83.
- Westreich R, Sampson I, Shaari CM, et al. Negative-pressure pulmonary edema after routine septorhinoplasty: discussion of pathophysiology, treatment, and prevention. Arch Facial Plast Surg. 2006 Jan-Feb;8(1):8-15.
- Aydin E, Quliyev H, Cinar C, et al. Eagle Syndrome Presenting with Neurological Symptoms. Turk Neurosurg. 2018;28(2):219-225.