Full HTML
Zenker’s diverticulum
Qian Hu1,2,3, Shi-Hua Zheng1,2,3, Wei Liu1,2,3
Author Affiliation
1Professor of Medicine, Departmnet of Gastroenterology, The First College of Clinical Medical Science,
2Institute of Digestive Disease, China Three Gorges University,
3Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
Abstract
A 77-year-old man presented to the gastroenterology clinic with a 1-year history of progressively worsening dysphagia to solids and liquids, weight loss, and regurgitation. His medical history was notable for mild chronic obstructive pulmonary disease. Physical examination showed no palpable cervical mass.
DOI: 10.32677/yjm.v2i2.3786
Pages: 115-115
View: 7
Download: 15
DOI URL: https://doi.org/10.32677/yjm.v2i2.3786
Publish Date: 28-09-2023
Full Text
A 77-year-old man presented to the gastroenterology clinic with a 1-year history of progressively worsening dysphagia to solids and liquids, weight loss, and regurgitation. His medical history was notable for mild chronic obstructive pulmonary disease. Physical examination showed no palpable cervical mass. Barium swallow examination revealed the presence of a 1.5 × 3.0 × 2.0 cm pharyngoesophageal diverticulum with contrast preferentially filling the diverticulum in the upper esophagus (Fig. 1a). Esophagogastroduodenoscopy confirmed the presence of the large, wide-mouthed pharyngoesophageal diverticulum, or Zenker’s diverticulum (Fig. 1b). As a relatively uncommon disorder occurring in older men, Zenker’s diverticulum is a posterior pharyngoesophageal pouch forming through pulsion forces in an area of relative hypopharyngeal wall weakness [1]. The underlying pathophysiological mechanism is fuzzy. Poor upper esophageal sphincter compliance may cause a high-pressure zone resulting in increased pulsion forces and subsequent Zenker’s diverticulum formation [2]. Because it can be clinically silent and individuals may not seek medical care, the true incidence of Zenker’s diverticulum is unclear. Symptoms predominantly include dysphagia, weight loss, and food regurgitation, which is due to cricopharyngeal dysfunction and filling of the false diverticulum during meals, causing compression of the anterior esophagus [3]. Therapeutic strategies for Zenker’s diverticulum mainly include surgical diverticulectomy and flexible endoscopic diverticulectomy, whose goal is severing of the septum between the esophageal lumen and the diverticulum containing the cricopharyngeal muscle. An endoscopic Zenker’s diverticulectomy was performed for him. The patient remained asymptomatic at a follow-up visit 1 year later.
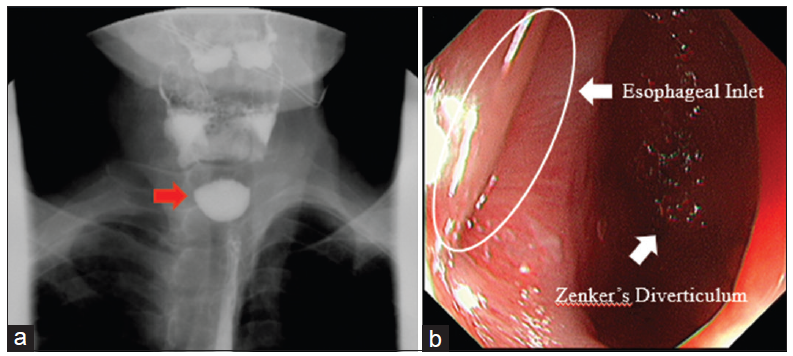
Figure 1: Zenker’s diverticulum. (a) Barium swallow examination showed the presence of a pharyngoesophageal diverticulum with contrast preferentially filling the diverticulum in the upper esophagus. (b) Upper gastrointestinal endoscopy confirmed presence of the large, wide mouthed Zenker’s diverticulum
Learning points
• Gastroenterologists should bear in mind Zenker’s Diverticulum whenever having a case of dysphagia.
• Barium swallow should be the first modality of investigation.
• Endoscopy should be carried out to confirm the diagnosis.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for publication of this manuscript and all accompanying images. The patient understands that while every effort is made to maintain the confidentiality of their identity, names, and initials, anonymity cannot be guaranteed.
AUTHORS’ CONTRIBUTIONS
All authors contributed to the completion of this work. The final manuscript was read and approved by all author
References
1. Law R, Katzka DA, Baron TH. Zenker’s diverticulum. Clin Gastroenterol Hepatol 2014;12:1773-82.
2. Le Mouel JP, Fumery M. Zenker’s diverticulum. N Engl J Med 2017;377:e31.
3. Eaton J, Limsui D, Grover M. A man with dysphagia, aspiration, and hematemesis. Diagnosis: Hematemesis from a bleeding vessel in a large Zenker’s diverticulum. Gastroenterology 2011;140:e11-2.