Full HTML
Prevalence of Depressive symptoms Among Elderly People Attending Primary Health Care Centers in Port Said Governorate, Egypt
Hazem Ahmed Sayed Ahmed1, Tarek Ibrahim Rashad El-Said1, Ahmed Mahmoud Mostafa1, Ismail Mohamed Youssef2
Author Affiliation
1Consultant, Department of Family Medicine, Faculty of Medicine, Suez Canal University, Suez, Egypt,
2Consultant, Department of Neuro-psychiatry, Faculty of Medicine, Suez Canal University, Suez, Egypt
Abstract
Background: Although geriatric depression is widespread in primary health care (PHC), local studies on the prevalence of depression in elderly PHC patients appear to be scarce. This study aimed to determine the prevalence of depressive symptoms and some of the associated risk factors among elderly PHC patients. Methods: A cross-sectional study recruiting elderly people (60 years or older) from five PHC centers in Port Said Governorate was conducted. All participants had a structured interview. The long version of the Geriatric Depression Scale (GDS) (cut-off point ≥10) was used in elders with a Mini-Mental State Examination (MMSE) ≥ 24. Results: About two-thirds of the total sample (65.7%) was females. The total prevalence of depressive symptoms was 49.4% of all subjects, more commonly in women (58.1% versus 32.8%). Multiple regression analysis shows that female gender, high education, unemployment, low income, lonely life, loss of a close person, chronic diseases, tumor, iatrogenic medications and depression history were the significant associated risk factors of depression in the studied elders after adjusting all previous variables in addition to age and marital status. Conclusion: Depressive symptoms constitute a significant health problem among older PHC patients in the Port Said governorate. Routine screening for depression of every elderly PHC patient is recommended for early detection.
DOI: 10.32677/yjm.v2i1.3893
Keywords: Depression, Elderly people, Geriatric depression scale, Primary health care
Pages: 37-43
View: 7
Download: 21
DOI URL: https://doi.org/10.32677/yjm.v2i1.3893
Publish Date: 10-05-2023
Full Text
Introduction
In Egypt, the last Census by the Central Agency for Public Mobilization and Statistics showed that the number of elders (60 years or older) was 6.9 million, which represented 6.6% of the total population. [1] Depressive symptoms are highly prevalent in late life, particularly among older primary care patients. [2] The international studies carried out in primary care settings report a wide range in the prevalence rates among elderly persons: major depression 1.0% to 22.4% and minor depression 5.2% to 36%. [3]
Depressive symptoms were present in about 15% of all elderly persons in the community and among nursing home residents [4] and among 60% of attendants' elders of outpatient psychiatric clinics in Egypt. [5] The percentage of depressive symptoms was 52.1% among elders in El-Nahda city [6], while it was 4.8% among the population of Amer-village, Suez governorate. [7] The risk factors for depression among older primary care patients were depression population, chronic medical illness, female gender, single or divorced state, brain disease, certain medication use and stressful life events. [8] Depression in older persons is associated with substantially reduced quality of life, increased mortality and increased use of all health and social service resources, including Primary Health Care (PHC). [3]
Despite the common occurrence of depression in elderly persons, its recognition remains a problem. The frequent atypical presentation of depressive disorders in older persons, the resistance of many elderly people to acknowledging and reporting their symptoms to their primary care physician, and the increasing pressure on primary care physicians to spend less time with their patients contribute to the low recognition rate of depression in this age group. [9]
Studies on the prevalence of depression among older primary care patients locally seem to be scarce. Most studies have been conducted in community settings, outpatient psychiatric clinics or nursing homes, leading to results that cannot be translated to the primary care settings.
This study aims to determine the prevalence of depressive symptoms and some of its associated risk factors among the elderly people who attend PHC centers in the Port Said governorate.
MATERIALS AND Methods
Design and Setting
A descriptive cross-sectional study was carried out in five PHC centers in Port Said governorate (Omr Ebn El-Khtab, Osman Ebn Afan, El-Manakh, El-Arab and El-Kabouty PHC centers) during the period March–November 2007.
Study population
The population was of elderly persons who were 60 years of age or above, attending PHC centers in Port Said governorate without severe hearing impairment, weak vision, schizophrenia or other psychotic disorders. The Mini-Mental State Examination score (MMSE) was expected to be <24. Participation in the study had to be voluntary. [10] The target sample was 196 elders but the studied elders were 178.
Sample technique and sampling
Five PHC centers were selected randomly. Within each center, all persons matching the inclusion and exclusion criteria were recruited until the total target sample size was reached. A relatively equal distribution of the number of persons within each center was maintained. The researcher assured that there was no contamination in the sampling.
Tools
The subjects were interviewed using a structured interview questionnaire to collect the following data:
A. Socio-demographic data: Every elder was asked about his/her age in years, marital status, educational status, occupation and loss of a close person during the past months.
B. Economic data: Every elder was asked about his/her monthly income: sufficient or not (according to their perception).
C. The medical history: Every elder was asked about his/her history of depression, hypertension, ischemic heart disease, diabetes mellitus, cerebrovascular stroke, urinary incontinence, tumor and other medical conditions (based on their previous diagnosis and drugs). Every elder was asked about his/her medication history
The Mini-Mental State Examination10 was used. As the sensitivity of the GDS [11] diminishes in patients with MMSE score <24, we excluded those elders. The 30-item GDS was used to determine the depressive symptoms and their severity. The yes-or-no questionnaire was administered orally, and one point was scored for each answer in parentheses. A score of 10 or more indicates depression (84% sensitivity and 95% specificity). Original scoring for the scale: one point for each of these answers. Cutoff: normal 0–9, mild depressives 10–19, and severe depressives 20–30. It was translated in slang Arabic language and validated by El-Banoby et al. [6]
Statistical analysis
Data were analyzed using the SPSS and EPI-Info statistical packages. The chi-squared test or Fisher exact test was used as appropriate to compare categorical data, and the Student t-test was used to compare quantitative data. The chi-squared test for linear trends was used to establish whether increasing risk levels were associated with depression. To estimate the independent association of each risk factor with depression, multiple regression analysis was performed. P-values < 0.05 were considered significant.
Ethical consideration
Approval for the research was obtained from the Ethics Committee of the Faculty of Medicine, Suez Canal University. After each participant had been fully informed of the goals and significance of the current study through an informed consent process, their verbal consent was obtained before the interview.
Results
Sample characteristics
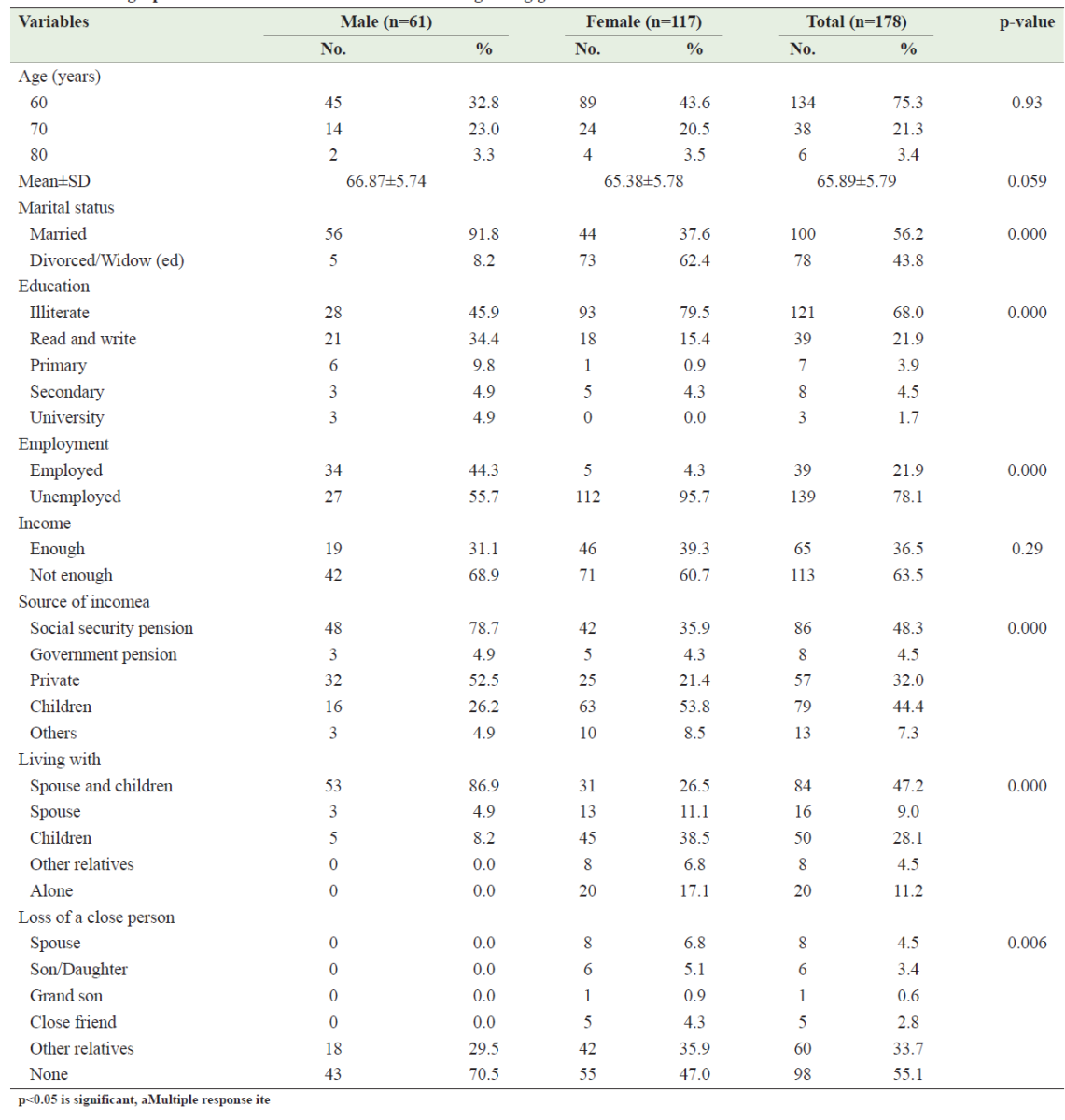
This study included 178 older PHC patients (60 years or older). Of the total sample, 117 (65.7%) were females. The demographic characteristics of the studied elders according to gender are shown in table 1. Approximately, three-quarters of all elders (75.3%) were 60–69 years, while only 3.4% of elders were 80 years or older. More than half of the studied elders (56.2%) were married, and 61.5% of elderly women were widowed. Approximately two-thirds of elders (68%) were illiterate. More women (79.5%) were illiterate compared to men (45.9%). More than half of the studied male elders (55.7%) were unemployed, and almost all women (95.7%) were unemployed.
The income was insufficient (according to elders' perceptions) in 63.5% of all elders. The main sources of income for the elderly were social security pension, children support and private income. About more than one-third of female elders (38.5%) were living with their children, and 17.1% of elders lived alone. About 30% of male elders had lost a close person while the corresponding percentage for female elders was 53%.
Table 1: Demographic characteristics of the studied elders regarding gender
Prevalence of depressive symptoms among the studied elder
Table 2 shows that 76 participants (42.7%) had GDS scores of 10–19, indicating mild depressive symptoms, while 12 (6.7%) had scores of 20–30 indicating severe depressive symptoms; these two groups were aggregated, giving a prevalence of 49.4%. The prevalence of depressive symptoms was significantly higher in females (58.1%) than in males (32.8%).
Table 2: Prevalence of depressive symptoms among the studied elders according to gend

Table 3 shows that elders with depressive symptoms had a significantly higher educational level than non-depressed ones had (39.8% vs. 24.4%, respectively). Unemployment was higher in the elders with depressive symptoms than those without (87.5% vs. 68.9%, respectively). It can be noticed that insufficient income was significantly higher in the elders with depressive symptoms than those without (75% vs. 52.2%). Living alone was more common in the elders with depressive symptoms than those without (17% vs. 5.6%). Loss of close persons was significantly higher in the elders with depressive symptoms than in non-depressed elders (P<0.01).
Tumors and use of iatrogenic medications were significantly higher in the elders with depressive symptoms than those without (p<0.01). Elders with depressive symptoms had a significantly positive past history of depression than those without (20.5% vs. 3.3%, respectively).
Table 3: Association between depressive symptoms and some associated risk factors among the studied elders

Table 4 shows that elders with depressive symptoms had a significantly higher prevalence of chronic diseases than those without (97.7% vs. 80%, respectively). Hypertension and diabetes mellitus were significantly higher in the elders with depressive symptoms than those without (p<0.01) but no statistically significant differences were observed between the two groups in ischemic heart diseases, chronic heart failure, cerebrovascular stroke and asthma/COPD. Arthritis and urinary incontinence were significantly higher in the elders with depressive symptoms than those without (p<0.01).
Table 4: Association between depressive symptoms and some co‑morbid conditions among the elderly subjects

Table 5 shows that female gender, high education, unemployment, low income, living alone, loss of a close person, presence of chronic diseases, tumor, iatrogenic medications and past history of depression were significant associated risk factors of depression in the studied elders as identified in the multiple regression analysis. It also shows that the 12 variables jointly contributed to 38.3 of the variance in the total score.
Table 5: Multiple regression analysis of depressed scores and certain independent risk factors

Discussion
In the current study, the 178 participants were aged 60 years. About 60% of participants were female, probably because women visit physicians more than men, and most of the studied elderly females were housewives. This ratio was consistent with Iliffe et al., who found that 65.3% of the 239 elderly participants were women.[12]
In the current study, depressive symptoms were present in 49.4% of all subjects. The higher prevalence rate might be because the elders in this study were unemployed with low income, loss of close persons and more comorbid conditions. This finding was consistent with Tai-Seale et al. [13], who reported that about 50% of older primary care patients had depression.
This rate was higher than Iliffe [12] and Weyerer [14], who reported that depression among older primary care patients was 21.8% and 11 to 29%, respectively, probably because of the used definition of depression and methodological variation among these studies. This rate was 10 times more than the prevalence of depression in Saber's study [7], which reported that depression affected only 4.8% of the elders, probably because it was a household study, i.e., a population not seeking medical care or advice, and it was conducted in a rural area with less stress, more religion, and more family and social support, which could have underestimated the prevalence. He also used the Even Briefer Assessment Scale for depression. [15]
The prevalence of depressive symptoms in the current study was more common in women (58.1% vs. 32.8%). This result agreed with that of Licht-Strunk et al., [3] Barry [16] and Weyerer [14], who reported a significant association between depression and elderly females in primary care settings.
In this study, no statistically significant correlation was found between depressive symptoms and age This finding was also consistent with El-Banoby et al.'s finding. [6]
In the current study, the depressed elders had significantly higher educational levels than the non-depressed ones had (39.8% vs. 24.4%, respectively). This finding could be explained by the notion that people with higher education could have higher expectations, failure to meet which could result in dissatisfaction, hence, the higher frequency of depressive symptoms. This finding was inconsistent with that of Abolfotouh et al. [15], who reported that uneducated subjects were five times more likely to have depression than those educated were. So a further study for verification of this result is needed, whether education per se is a strong risk factor for depression or it produces effects inconsistent with other factors.
In this study, unemployment was higher in the elders with depressive symptoms than those without (87.5% vs. 68.9%, respectively). Retirement as a variable, in particular, was not studied in this study as it is assumed that the retired elderly may have easy access to insurance hospital services more than to PHC services.
In the current study, we found that insufficient income was significantly higher in the elders with depressive symptoms than those without (75% vs. 52.2%). This correlated with the finding of El-Banoby et al. [6]
In the current study, living alone was more common in the elders with depressive symptoms than those without (17% vs. 5.6%). This result agreed with the results of Weyerer et al., who found that the prevalence of depression among the non-demented primary care attenders was significantly higher among those living alone (11.2%) compared to those not living alone (8.0%). [14] This result was consistent with the results of El-Banoby et al., 6 Saber7 and Abolfotouh et al. [15]
In this study, we found that losing a close person was significantly higher in the elders with depressive symptoms than in non-depressed elders (P<0.01). This result was consistent with the results of El-Banoby et al. [6] and Saber. [7]
In the current study, approximately 70.5% of elders with depressive symptoms had hypertension, and 70.5% had diabetes mellitus. These findings were higher than those in other local studies. These differences were probably because the majority of the subjects in the current study attended the PHC centers for monthly treatment refills of hypertension and diabetes mellitus.
In the current study, no statistically significant differences were observed between depressed and non-depressed elders regarding cerebrovascular stroke. This finding was inconsistent with the vascular depression hypothesis. [17] This difference might be due to the small number of the studied elders with cerebrovascular stroke and also as a result of the exclusion of impaired cognitive elders from sampling, so further research is needed to study this association.
This study revealed an association between depressive symptoms and hypertension, diabetes mellitus and arthritis. This association might be due to merely a coexisting association, fear of or produce chronic pain disability and some of the drugs, which could be used to treat these medical conditions, can cause symptoms and signs of depression.
Conner et al. reported that depression may be a serious consequence of urinary incontinence. [18] In the current study, we found a significant association between depressive symptoms and urinary incontinence, probably because the affected persons perceive it to be very embarrassing and may isolate themselves from society leading to social anxiety and emotional problems such as depression.
This study has several limitations. First, it is not designed to examine cause-and-effect relationships; it can suggest only one association. Second, the assessment of medical conditions was limited to self-reporting by the elders. Third, the data was old and predated the events of January 25, 2011. However, due to the lack of studies in this field, this study can serve as a reference for future work.
CONCLUSION
Depressive symptoms are a significant health problem among elderly PHC patients in Port Said Governorate. Routine screening for depression in any elderly PHC patient is recommended for early detection.
AUTHORS’ CONTRIBUTION
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; and gave final approval of the version to be published.
References
- Central Agency for Public Mobilization and Statistic Annual Report. Cairo, Central Agency for Public Mobilization and Statistic, 2022. https://www.capmas.gov.eg/Admin/News/PressRelease/2022929134228_333.pdf [last accessed on January 2023]
- Alexopoulos GS, Borson S, Cuthbert BN. et al. Assessment of Late Life Depression. Biol Psychiatry 2002;52:164–174.
- Licht-Strunk E, van der Kooy KG, van Schaik DJF, et al. Prevalence of depression in older patients consulting their general practitioner in The Netherlands. Int J Geriatr Psychiatry 2005; 20: 1013-1019.
- Morsy N.M. Effect of Institutionalization on Elderly, feeling of Depression. In: Elderly on Arabic World (the current status and future), Hellwan press,
- Abou-Hatab. Trends in Geriatric Research: the current status and future directions: the case of
- El-Banoby MH, Metwally A, Mortagy A, et al. Prevalence of Depression Among Egyptian Geriatric Community. MD. Thesis, Faculty of Medicine,
- Saber M. Household study of common health problems among elders in Amer-village of
- Boswell EB, Stoudemire A. Major depression in the primary care setting. American J Medicine 1996; 101: 35-95.
- Lapid M., Rummans T. Evaluation and Management of Geriatric Depression in Primary Care. Mayo Clin. Proc. 2003;78: 1423-29.
- Folstein MF, Folstein SE, McHugh PR. ‘
- Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatry Res 1982; 17: 37-49.
- Iliffe SR, Tai S, Haines AP, et al. Assessment of elderly people in general practice. Depression, functional ability and contact with services. British Journal of General Practice, 1993; 43: 371-374.
- Tai-Seale M, McGuire T, Colenda C, et al. Two-Minute Mental Health Care for Elderly Patients: Inside Primary Care Visits. J Am Geriatr Soc. 2007; 55(12): 1903-1911.
- Weyerer S., Eifflaender-Gorfer S.et al. Prevalence and risk factors for depression in non-demented primary care attenders aged 75 years and older. Journal of Affective Disorders 2008.
- Abolfotouh MA, Daffallah AA, Khan MY, et al. Psychosocial assessment of geriatric subjects in Abha City, Saudi Arabia. Eastern Mediterranean Health Journal.2001;7 (3), 481-491
- Barry K, Fleming M, Manwell L, et al. Prevalence of and Factors Associated With Current and Lifetime Depression in Older Adult Primary Care Patients. Fam Med 1998; 30 (5): 366-71.
- Alexopoulos G, Bruce M, Silbersweig D, et al. Vascular depression: a new view of late-onset depression. Dialogues in Clinical neuroscience 1999; 1 (2): 68-80.
- Conner E. Lind L. Urinary incontinence in nursing homes: Epidemiology and management guidelines. Prim Care Update Ob/Gyns 2001; 8: 248–252.