Full HTML
Utility of The MGIT 960 TB System For Recovery of Mycobacteria
Amara Esther Ulasi1, Ndubuisi Obiora Nwachukwu2, Reginald Azu Onyeagba3, Solomon Nnanna Umeham4, Anuli Amadi5
Author Affiliation
1Researcher, 4Professor of Biology, Department of Animal and Environmental Biology,
2Researcher, Department of Medical Laboratory Science,
3Professor of Microbiology, Department of Microbiology,
4Professor of biology, Department of Animal and Environmental Biology, Abia State University, PMB 2000, Uturu,
5Researcher, Department of Mycobacteriology, South East Zonal TB Reference Laboratory, Amachara Specialist Hospital, Umuahia, Abia, Nigeria
Abstract
Background and Objectives: Pulmonary tuberculosis remains a public health issue in Nigeria. The rapid diagnosis of pulmonary tuberculosis is essential for the early initiation of treatment and management of patients. The utility of the BACTEC MGIT 960 TB system was evaluated and compared with the Lowenstein Jensen (LJ) culture method for the recovery of Mycobacteria from sputum samples. Methods: A total of 2400 sputum samples submitted to the South East TB Zonal Reference Laboratory, Amachara Umuahia, Nigeria were tested. Samples were decontaminated using the standard N-Acetyl-L-Cysteine Sodium Hydroxide method and concentrated prior to processing. The processed samples were inoculated into both MGIT 960 tubes and LJ medium and incubated accordingly. Results: From all sputum samples, Mycobacteria were recovered from 201(8.4%) sputum samples by the MGIT 960 system and 175(7.3%) by LJ culture (P 0.014). The sensitivity for MGIT and LJ culture for mycobacteria were 95.0% and 80.1% respectively. Among the 201 MGIT-positive cultures, 127(63.2%) were identified as Mycobacterium tuberculosis complex (MBTC) and 74(36.8%) as Mycobacteria other than tuberculosis ( MOTT). The recovery rate of MTBC from LJ-positive samples was 84.0% and MOTT 16.0%. MGIT 960 identified more MOTT than LJ culture(P 0.045). The contamination rate associated with MGIT and LJ culture was 4.1% and 2.5% respectively(P 0.037). The time to detection of mycobacteria in MGIT 960 and LJ was 14.8 days and 33.2 days respectively. Conclusion: MGIT 960 has good diagnostic accuracy. It provided a more rapid and higher recovery of all mycobacteria than the LJ culture.
DOI: 10.32677/yjm.v2i1.3877
Keywords: BACTEC MGIT 960, Comparison, Lowenstein Jensen, Mycobacterium tuberculosis
Pages: 30-32
View: 8
Download: 15
DOI URL: https://doi.org/10.32677/yjm.v2i1.3877
Publish Date: 10-05-2023
Full Text
Introduction
Pulmonary tuberculosis (PTB) is a major public health problem with significant morbidity and mortality. [1] Rapid and accurate diagnosis of active pulmonary tuberculosis, especially in developing countries, is a major challenge to global control of the disease. [2,3]
Most developing countries rely on the conventional Lowenstein- Jensen’s (LJ) culture and microscopy (Ziehl-Neelsen method) for the detection of Mycobacterium tuberculosis. The LJ culture has a long duration to detection and Ziehl-Neelsen (ZN) has low sensitivity. [4]
We, therefore, evaluated the accuracy of the MGIT 960 TB system for the recovery of mycobacteria and compared it with the conventional LJ culture to ascertain its utility.
MATERIALS AND METHODS
Settings: This prospective study was conducted at the South East Zonal TB Reference Laboratory of Amachara Specialist Hospital, Umuahia, Abia State, Nigeria between September 2020 and August 2021. The Reference Laboratory receives samples from all five South-Eastern States TB Control Program for culture and drug susceptibility testing. The sputum samples were from presumptive TB patients who had been tested using Microscopy(ZN Methods).
Study Population: A total of 2400 sputum samples were enrolled for the study. The age and sex of the patients were omitted. We excluded all samples for Line Probe Assay and Drug Susceptibility testing. All samples for LJ culture were included.
Decontamination and Processing of Samples:
All samples were decontaminated by the standard N-acetyl-L-cysteine (NALC)- Sodium hydroxide (NaOH) method and concentrated before processing [5] Each sample was diluted with an equal volume of 4% NaOH and 0.5ml NALC and mixed properly. Then centrifuged at 3000 r.p.m for 15 minutes. The sediment was suspended in 1ml of sterile Phosphate-buffered saline, pH 6.8, and used for further analysis. Exactly 0.5ml of the processed sample was inoculated into the MGIT 960 tube and 3 drops into the LJ medium. Two drops of the processed sample were placed on a slide to make a smear, stained by the ZN method for acid-fast bacilli (AFB).
Detection of Mycobacteria on MGIT 960 TB System
Before inoculation of samples into a 7ml MGIT tube, the MGIT PANTA antibiotic mixture was reconstituted with 15ml MGIT growth supplement and mixed to complete dissolution, giving a clear solution. To the 7ml MGIT tube, 0.8ml of this enrichment was added followed by 0.5ml of the processed sample, and the tube was recapped immediately. The contents were mixed by inverting the tube 3 times. All inoculated MGIT tubes were incubated at 37oC in the BACTEC MGIT 960 instrument after scanning the bar code. The tubes were incubated until they were flagged positive by the instrument or for the duration of the recommended 42 days.[6] Tubes signaled positive for growth were removed from the instrument and observed visually under the light. Mycobacterial growth appears grandular in shape, settling at the bottom of the tube while contaminating bacterial growth appears as uniform turbidity in the entire tube.
All MGIT 960 positive tubes were stained by the ZN method for acid-fast bacilli and sub-cultured on Blood agar.
Identification of Mycobacterium Tuberculosis Complex by MGIT 960 using SD Bioline TB Antigen MPT64 RAPID test
The MPT64 protein detection-based immune-chromatographic test (SD Bioline Kit, Standard Diagnostic Inc, Korea) is a specific antigen that differentiates MTBC from the Mycobacteria other than the tuberculosis (MOTT) group. [7,8] It was performed on AFB-positive MGIT cultures as described by the manufacturer. [7] Results were recorded accordingly.
Isolation and identification of Mycobacterium tuberculosis by Lowenstein Jensen (LJ) Culture Method
Exactly 2 drops of the processed sample were inoculated onto a properly labeled LJ slant, using a sterile pipette. The inoculated slants were incubated at 37oC for up to eight weeks in a vertical position. The LJ slants were observed daily for the first week and thereafter once a week for 8 weeks for the visible appearance of colonies. Contaminated cultures and LJ media which liquefied or turned a dark green were discarded. [5]
The slants which showed growth within one week of incubation were regarded as rapid growers, i.e. Mycobacteria other than tuberculosis (MOTT). Colonies developing post 2-6 weeks were considered slow-growing and termed the Mycobacterium tuberculosis complex. Colonial morphology was also used in characterization. [5,9]
Ethical Approval and Patient consent:
Ethical approval was obtained from the Health and Ethics Committee of the Amachara Specialist Hospital, Umuahia, Abia State, Nigeria (Approval number: ASHU/020/0310).
Statistical Analysis: Data generated were analyzed using descriptive statistics and
categorical variables expressed in percentages. Differences
in proportions were compared using Chi-square. Level of
significance was set at P < 0.05(stating actual value). The sensitivity of each method was calculated
RESULTS
From all sputum samples, Mycobacteria were found in 201 (8.4%) samples by the MGIT 960 system and 175 (7.3%) by LJ culture (P=0.014). The sensitivity for MGIT 960 system and LJ culture for mycobacteria were 95.0% and 80.18% respectively. The contamination rate associated with MGIT 960 was significantly higher than LJ culture [4.1% vs 2.5 %, (P=0.037)] (Table 1)
Table 1: Recovery of mycobacteria by MGIT 960 and LJ culture, and identification of MTBC and MOTT from positive MGIT 960 samples and LJ culture
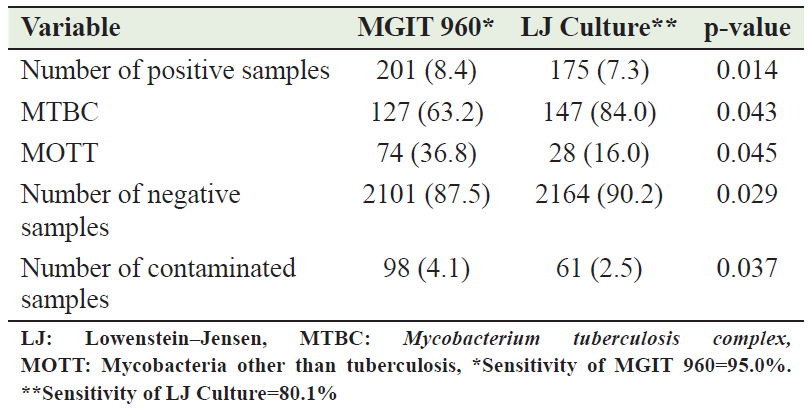
Among the 201 mycobacteria grown by MGIT 960 system, 127 (63.2%) were confirmed by SD Bioline MPT 64 RAPID test as MTBC, and 74 (36.8%) were identified as MOTT. Similarly, of the 174 mycobacteria grown by LJ culture, 147 (84.0%) were identified as MTBC and 28 (16.0%) as MOTT (Table 1). MGIT 960 identified more MOTT than the LJ culture (P=0.045). The time to detection of mycobacteria was 14.8 days in the MGIT 960 and 33.2 days in the LJ culture.
Discussion
Rapid diagnosis of pulmonary tuberculosis is essential for the treatment, prevention, and control of the disease. The capacity of laboratories to promptly identify cases of Mycobacterium tuberculosis from clinical samples is vital in the management of pulmonary tuberculosis patients. [10,11]
The liquid culture of mycobacteria is more sensitive than smear microscopy and more rapid than classical solid methods. [12]
In our study, the sensitivity of the MGIT 960 TB System for mycobacteria was 95.0% compared to 80.1% by LJ culture. A study conducted in India showed increased recovery of mycobacteria by MGIT 960 (94.1%) compared to LJ (89.0%). [13] Several other studies had similarly reported higher recovery rates of mycobacteria ranging from 80% - 100% for MGIT 960 and 44% - 93% LJ culture. [6,12, 14]
Exactly 63.2% of all MGIT 960 positive mycobacteria were identified as mycobacteria tuberculosis complex in our study. The LJ culture identified 84% as MTBC. The difference (20.8%) could be attributed to contamination as MGIT 960 medium is rich in proteins.
It was observed that MGIT 960 system detected MOTT (36.8%) more rapidly than the LJ (16.0%). This may be because MOTT survived the decontamination process. [15] In their study in Bangladesh, the MGIT 960 method similarly detected non-tubercular mycobacteria (91.7%) more effectively than the LJ culture.[ 14]
Out of the 2400 sputum samples analyzed, the contamination rate was higher (4.1%) in the MGIT 960 method compared to 2.1% in LJ. This is consistent with the previous studies. Hasan et al [19] showed a higher contamination rate with MGIT 960 (9.5%) than with LJ culture (1.3%). Earlier Studies [22, 23] reported a higher contamination rate with MGIT 960. [16,17] In contrast to our findings, a lower contamination rate was reported with MGIT 960 than with LJ.[18] MGIT 960 liquid culture requires careful processing and handling of samples.
The median time to detection of mycobacteria was found to be 13.8 days with MGIT 960 and 33.2 days with LJ method. There was a significantly shorter time with MGIT 960. This is in line with 18.2 days with MGIT 960 and 32.5 days with LJ previously observed. [12,19,20]
Conclusion
MGIT 960 TB system is a utility method. It provides a more rapid and higher recovery of all mycobacterial (MTBC and MOTT) than LJ culture. It could be used as the initial test for the diagnosis of pulmonary tuberculosis.
AUTHORS’ CONTRIBUTION
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; and gave final approval of the version to be published
References
- Gopalaswamy R, Sivakumar S, Rajesh M, et al. Of tuberculosis and non-tuberculous mycobacterial infections- a comparative analysis of epidemiology, diagnosis and treatment. J Biomed Sci 2020; 27: 1-7.
- Walis RS, Pai M, Menzies D, et al. Biomarkers and diagnosis for tuberculosis: progress, needs and translation into practice. Lancet 2010; 375: 1920- 1937.
- McNerney R, Daley P. Towards a point-of-care test for active tuberculosis: obstacles and opportunities. Nat Rev Microbiol 2011; 9: 204- 213.
- World Health Organization. Global Tuberculosis Control. 2011. Geneva, Switzerland.
- Munshi SK, Rahman F, Kamal SMM, et al. Comparison among different diagnostic methods used for detection of extra-pulmonary tuberculosis in Bangladesh. Int J Mycobacteriol 2012; 1: 190- 195.
- Satti L, Ikram A, Abbasi S, et al. Evaluation of BACTEC MGIT 960 system for recovery of MTBC in Pakistan. Malaysian J Microbiol 2010; 6(2): 203- 208.
- Hasegawa N, Miura T, Ishii K, et al. New simple and rapid test for culture of Mycobacterium tuberculosis: a multicenter study. J Clin Microbiol 2002; 40: 908- 912.
- Maura AK, Nag VL, Kushwaha RA, et al. Evaluation of an immunochromatographic test for discrimination between Mycobacterium tuberculosis complex and Non-tubercular mycobacteria in clinical isolates from extra-pulmonary tuberculosis. Indian J Med Res 2012;135: 901- 906.
- Rahman F,Munshi SK, Kamai SMM, et al. Comparison of different microscopic methods with conventional tuberculosis cultures. S J Microbio; 2011; 1(1): 46- 50.
- Balaji S, Gomathi S, Devi S, et al. Reprocessing of contaminated MGIT 960 cultures to improve availability of valid results for mycobacteria. Int J Microbiol 2020;3: 1- 3.
- Arora J, Gavish K, Ajoy KW, et al. Utility of MPT64 antigen detection for rapid confirmation of Mycobacterium tuberculosis complex. J Global Infect Dis 2015; 7(2): 66 -69.
- Kalpana T, Imola J, Ellappan K, et al. Comparison of MGIT 960 with Lowestein-Jensen method for mycobacteria detection in pulmonary tuberculosis and drug susceptibility testing. Acta Scientific Microbiol 2021; 4(6); 12- 17.
- Sharma S and Dhar R. Non-tuberculous mycobacterial diseases: current diagnosis and treatment. Astrocyte 2017,4: 67- 74.
- KohWZ, Ko Y, Kim C, et al. Rapid diagnosis of tuberculosis and multidrug-resistance using a MGIT 960 system. Ann Lab Med 2012; 32(4): 264- 269.
- Abdel-Aziz N, Hydi A, Mohammed MM, et al. A comparative evaluation of the BACTEC MGIT 960( Mycobacterium Growth Indicator Tube) system with Lowestein –Jensen solid medium for diagnosis of pulmonary tuberculosis. Egyptian J Microbiol 2009; 9: 204- 213.
- Somoskovi A, Kodmon C, Lantos A, et al. Evaluation and clinical usefulness of BACTEC MGIT 960. J Clin Microbiol 2000; 38(6): 2395- 2397
- Hanna BA, Ebrahimzadeh A, Elliot LB. Multicenter evaluation of the BACTEC MGIT 960 system for recovery of mycobacteria. J Clin Microbiol 1997; 37: 748- 752.
- Deepali S, Amit S, Adesh K, et al. Comparison of BACTEC MGIT with conventional methods for detection of mycobacteria in clinical suspected patients of extra-pulmonary tuberculosis in tertiary care hospital. Int J Res Med Sci 2017; 5: 3530- 3533.
- Diriba G, Abebaw K, Zelalum Y, et al. Performance of Mycobacterium Growth Indicator Tube BACTEC 960 with Lowestein-Jensen method for diagnosis of Mycobacterium tuberculosois at Ethiopian National Tuberculosis Laboratory, Addis Ababa, Ethiopia. BMC Research Notes 2017, 10: 181.
- Mishra V, Sami H, Bareja R, et al. Evaluation of MGIT over other phenotypic methods for the detection of pulmonary and extra-pulmonary tuberculosis at tertiary care center in North India. Int J Pharma Sci Res 2016; 7: 2568.