Full HTML
The prevalence of and risk factors for stroke among type 2 diabetes mellitus patients in Qatar: A hospital-based study
Gowri Karuppasamy1 , Shaikha Al Shokri1 , Aseel Sukik1 , Khaled Abdul-Kader Bacha2
Author Affiliation
1Consultant,
2 Intern Department of Medicine, Hamad General Hospital, Doha, Qatar
Abstract
Background and Objectives: The complications of type 2 diabetes mellitus (T2DM) can occur in some organs, such as the heart, blood vessels, eyes, kidneys, and nerves. Stroke, one of such complications, is increasing every year. This study aims to investigate the prevalence of and risk factors for stroke among T2DM patients in Qatar.
Methods: This was a secondary post hoc analysis of collected data from our previous study titled “Association of Vitamin D deficiency with dyslipidemia, glycemic control, and microalbuminuria in patients with T2DM in Qatar.”
Results: The prevalence of stroke among our patients was3.8%. Acomparison between stroke and no-stroke groups showed a significant association between stroke and other diseases, namely, chronic kidney diseases (CKD) (p=0.007), coronary artery disease (CAD) (p=0.010), peripheral vascular disease (PVD) (p<0.001), retinopathy (p=0.044), prolonged duration of diabetes mellitus (DM) (p=0.041), glycated hemoglobin (HbA1c) (p=0.006), and a high serum creatinine level (p=0.003). In the multivariate analysis, we identified the following variables as independent risk factors for stroke in patients with T2DM: male gender, CKD, CAD, PVD, high HbA1c, a high creatinine level, and prolonged duration of DM.
Conclusion: The prevalence of stroke among T2DM patients in Qatar was around 3.8%. The main risk factors were male gender, CKD, CAD, PVD, high HbA1c, prolonged duration of DM, and a high level of creatinine.
DOI: 10.32677/yjm.v1i2.3637
Keywords: Logistic regression, Qatar, Risk factors, Stroke, Type 2 diabetes mellitus
Pages: 78-81
View: 8
Download: 18
DOI URL: https://doi.org/10.32677/yjm.v1i2.3637
Publish Date: 28-03-2025
Full Text
Diabetes is one of the most common non-communicable diseases and a growing global public health problem with a significant economic burden. Type 2 diabetes mellitus (T2DM) accounts for 90% of diabetes worldwide [1]. In chronic complications,such as chronic kidney diseases(CKD) and cardiovascular diseases,strokes are well-known outcomes of T2DM progression that reduces patients’ quality of life and increases the burden on the health-care system. Individuals with diabetes have a risk of experiencing a stroke 2 times higher than those that do not have this condition [2]. Some researchers estimated that the prevalence of stroke among T2DM patients was between 2.5% and 20% [2-4], while a recent meta-analysis estimated that the prevalence of diabetes in all stroke inpatients was 28% [5]. With a prevalence of approximately 19.8%, Qatar is among the top 10 nations in the world for diabetes. As Qatar continues to develop, the risk of diabetes is increasing due to ongoing urbanization and changing lifestyles in the country [1]. A recent study [6] shows that about 71.8% of stroke patients in Qatar have diabetes mellitus (DM). The prevalence of stroke among T2DM patients in Qatar is not well-studied. This study aimed to investigate the prevalence of and risk factors for stroke among T2DM patients in Qatar.
MATERIALS AND METHODS
Study Design, Setting, and Population
This was a secondary post hoc analysis of collecteddatafromour previous study titled “Association of Vitamin D deficiency with dyslipidemia, glycemic control, andmicroalbuminuriainpatients with T2DMin Qatar” [7], which was conductedfromJanuary1,to July 31, 2018. The collected data were usedtoconductanewstudy with modified objectives, without usingpatients’medicalrecords.
Definitions, Inclusion and Exclusion Criteria
Stroke status was determined on the basis of the information gathered initially fromthe electronic medical recordsoftheinvolved patients. According to these records, strokeshadbeendiagnosedby the stroke teamin the hospital. However, theprimarystudydidnot gather information on types ofstrokes (ischemicorhemorrhagic). Therefore, no distinction was made regarding the types ofstroke in this study. The primary outcome of this study was the prevalence of stroke among T2DM, while the secondary outcomes were independent risk factors for stroke among T2DM patients.
Data Analysis
The data analysis was performed using the Statistical Package for the Social Sciences software V23 (IBM Corp., Armonk, NY, USA). To report data, mean and standard deviation were calculated for quantitative variables, whereas numbers and percentages were used for qualitative variables. The Fisher exact test and analysis of variance test were used for cross tabulation at 0.05 margins of error. Variables with p<0.05 values were entered into the multiple logistic regression model to identify the risk factors for stroke among our patients. All significance tests were two-sided with p<0.05 as the level of significance.
Ethical Consideration
Since this was a secondary post hoc analysis of collected data from our previous study, ethics committee approval or informed consent was not required. The original study was approved by the medical research ethical committee at Hamad medical corporation, Qatar.
RESULTS
Demographic and Clinical Data
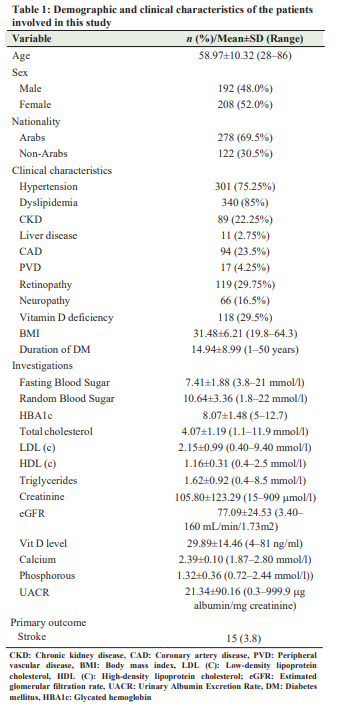
The primary study recruited 400 subjects with T2DM. Their mean age was 58.97±10.32 years (the range of 28–86 years), and the majority were women (52.0%) and Arabs (69.5%). The mean duration of type 2 diabetes diagnosis was 14.94±8.99 years (the range of 1–50 years), and mean BMI was 31.48±6.21 kg/m2 (the range of 19.8–64.3 kg/m2 ). Table 1 describesthe demographic and clinical characteristics of the study population. The prevalence of stroke among this cohort was 3.8%.
Comparison between Stroke and No-stroke Groups
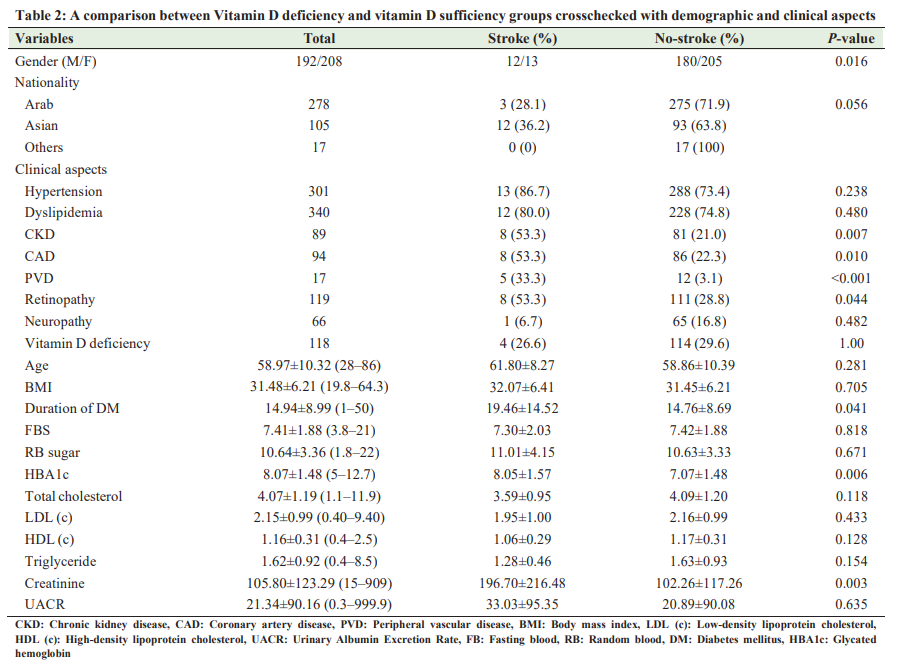
A comparison between stroke and no-stroke groups showed a significant association between stroke and other diseases, namely, chronic kidney CKD (p=0.007), coronary artery disease (CAD) (p=0.010), peripheral vascular disease (PVD) (p<0.001), retinopathy (p=0.044), prolonged duration of DM (p=0.041), glycated hemoglobin (HbA1c) (p=0.006), and a high serum creatinine level (p=0.003) (Table 2).
Multiple Regression Test to Identify the Risk Factors for Stroke
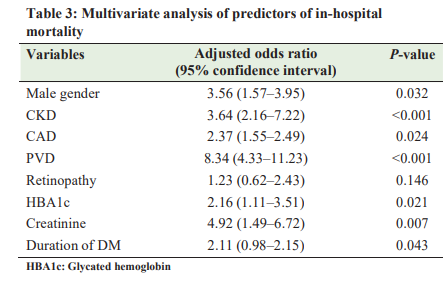
Table 3 demonstrates the association of various risk factors with stroke. In the multivariate analysis – after adjusting for various confounders, such as gender, CKD, CAD, PVD, retinopathy,
and a high serum creatinine level – we identified the following variables as independent risk factors for stroke in patients with T2DM: male gender, CKD, CAD, PVD, HbA1c, a high creatinine level, and prolonged duration of DM.
DISCUSSION
To the best of our knowledge, this is the first study conducted to investigate prevalence of stroke among T2DM patients in Qatar.
The prevalence of stroke among T2DM patients varies from country to country. Tseng et al. found the prevalence of 7.5% in Taiwan [8], while Almobarak et al. found the prevalence of 2.8% in Sudan [3]. Khan et al. found the prevalence of 11.2% in the United States [4], while Asfandiyarova et al. found the prevalence of 2.9% in Russia [9]. In Indonesia, Amelia et al. found that the prevalence was 20% [2], while, in Qatar, we found that the prevalence of stroke among T2DM patients was 3.8%. This variation can be attributed to the variation in the coexisting medical conditions, such as hypertension, CKD, and cardiovascular diseases [10]. Risk factors for stroke in T2DM patients have been identified in many studies. The identification of the risk factors proved invaluable as it could help prevent late complications of diabetes and reduce the mortality rate from stroke. In Qatar, no previous studies had investigated predictors of stroke among adults with T2DM; our study was the first to do that. Khan et al. and Tseng et al. identified hypertension as an independent risk factor for stroke among diabetic patients [4, 8]. According to a report by the American Heart Association (AHA), hypertension increased the risk of stroke by weakening arteries, and weakened arteries were more likely to burst or clog, resulting in hemorrhagic or ischemic stroke, respectively [11]. In contrast, we could not find hypertension as a predictor of stroke in our study. A study by Bushnell et al. reported that the risk of stroke doubled every 10 years after the age of 55 [12]. The possible mechanism underlying the effect of age was that arteries naturally became narrower and harder with increasing age due to the change mediated by endothelial dysfunction and impaired cerebral autoregulation [13]. In contrast, our study did not show a significant association between age and stroke. However, among our patients, male sex was found to be a risk factor for stroke. A study by Tseng et al. had similar findings [8]. DM is a major risk factor for stroke. Individuals with diabetes have a risk of experiencing a stroke 2 times higher than those that do not have this condition [4]. DM isstrongly associated with both microvascular and macrovascular complications. Microvascular complications include retinopathy, nephropathy, and neuropathy, while macrovascular complications include ischemic heart disease, PVD, and cerebrovascular disease. They result in organ and tissue damage in approximately one-third to half of people with diabetes [14]. Given that these complications are correlated with a history of poor blood glucose control, they may also be an indication of the effect of diabetes on the occurrence of stroke. The harmful effects can be explained not only by endothelial damage but also by factors such as hypertension which is often triggered by kidney damage. Similarly, the bivariate analysis in our study has shown a significant association between CKD, CAD, PVD, retinopathy, a high level of HbA1c, long duration of DM, and a high level of creatinine. Almobarak et al. found that HbA1c and the duration of diabetes were significantly associated with stroke. In multivariate analysis, we found CKD, CAD, PVD, a high level of HbA1c, duration of DM, and a high level of creatinine as independent risk factors for stroke. This study has some limitations. It is a post hoc analysis of a retrospective cohort study that was conducted at a single hospital. Amore comprehensive prospective study should be conducted for a more accurate estimation of prevalence and risk factors. Thisstudy is novel asit is the first that is conducted in Qatar. Our findings will be useful in guiding health equity programsthat are geared toward reducing strokes among populations with diabetesin Qatar
CONCLUSION
The prevalence of stroke among T2DM patients in Qatar was around 3.8%. The main risk factors were male gender, CKD, CAD, PVD, a high level of HbA1c, long duration of DM, and a high level of creatinine. Strict blood sugar control and regular screening for proteinuria could help reduce stroke risks in T2DM patients.
AUTHORS’ CONTRIBUTIONS
Karuppasamy G analyzed the data and wrote the final manuscript. Al Shokri S proposed the idea, reviewed the literature, and aided in the data analysis. Sukik A reviewed the literature and aided in writing the manuscript. Bacha KA aided in the data analysis, literature review, and the revision of the final manuscript. All authors read the manuscript and agree to its publication.
References
1. Butler J, Bourke PJ. Diabetes and stroke in Qatar: Results of a prospective stroke register. Int Diabetes Nurs 2015;12:63-8.
2. Amelia R, Harahap NS. Stroke among Type 2 diabetes mellitus patients at Haji Adam malik general hospital, Medan, Indonesia. Open Access Maced J Med Sci 2019;7:2643-6.
3. Almobarak AO, Badi S, Elmadhoun WM, et al. The prevalence and risk factors of stroke among Sudanese individuals with diabetes: Cross-sectional survey. Brain Circ 2020;6:26-30.
4. Khan MM, Roberson S, Reid K, et al. Prevalence and predictors of stroke among individuals with prediabetes and diabetes in Florida. BMC Public Health 2022;22:243.
5. Lau LH, Lew J, Borschmann K, et al. Prevalence of diabetes and its effects on stroke outcomes: A meta-analysis and literature review. J Diabetes Investig 2019;10:780-92.
6. Imam YZ, Kamran S, Saqqur M, et al. Stroke in the adult Qatari population (Q-stroke) a hospital-based retrospective cohort study. PLoS One 2020;15:e0238865.
7. Karuppasamy G, Al Shokri S, Sukik A, et al. Association of Vitamin D deficiency with dyslipidemia, glycemic control, and microalbuminuria in patients with Type 2 diabetes mellitus in Qatar. Yemen J Med 2022;1:17-21.
8. Tseng CH, Chong CK, Sheu JJ, et al. Prevalence and risk factors for stroke in Type 2 diabetic patients in Taiwan: A cross-sectional survey of a national sample by telephone interview. Diabet Med 2005;22:477-82.
9. Asfandiyarova NS, Kolcheva NG, Ryazantsev IV, et al. Risk factors for stroke in Type 2 diabetes mellitus. Diabetes Vasc Dis Res 2006;3:57-60.
10. Liao CC, Shih CC, Yeh CC, et al. Impact of diabetes on stroke risk and outcomes: Two nationwide retrospective cohort studies. Medicine (Baltimore) 2015;94:e2282.
11. American Heart Association. How High Blood Pressure can Lead to Stroke. United States: American Heart Association. Available from: https://www. heart.org/en/health-topics/high-blood-pressure/health-threats-from-highblood-pressure/how-high-blood-pressure-can-lead-to-stroke [Last accessed on 2022 Aug 30]
12. Bushnell C, McCullough LD, Awad IA, et al. Guidelines for the prevention of stroke in women. Stroke 2014;45:1545-88.
13. Yousufuddin M, Young N. Aging and ischemic stroke. Aging (Albany NY) 2019;11:2542-4.
14. Cade WT. Diabetes-related microvascular and macrovascular diseasesin the physical therapy setting. Phys Ther 2008;88:1322-35.