Full HTML
Determine the Relationship Between Hypertension and Uterine Fibroids
Md Sayed Ali Sheikh1, Umme Salma2
Author Affiliation
1 Associate Professor, Department of Internal Medicine, College of Medicine, Jouf University, Sakaka, Kingdom of Saudi Arabia
2 Associate Professor, Department of Obstetrics and Gynecology, College of Medicine, Jouf University, Sakaka, Kingdom of Saudi Arabia.
Abstract
Background: Numerous studies have linked uterine fibroids to hypertension, suggesting that this condition may be a risk factor unique to women. These days, fibroids are the main cause of myomectomy and hysterectomy. This study aimed to ascertain the relationship between uterine fibroids and hypertension in Saudi women.
Methods: This case-control study was carried out between January 2023 and January 2024 on patients with uterine fibroids and non-uterine fibroids who had an appointment for surgery at the gynecological department of the Maternal and Children Hospital (MCH) Sakaka, Aljouf, Saudi Arabia. Blood pressure readings and fibroid diameters are important factors in studying uterine fibroids.
Results: The 140 individuals who were split into 70 cases and 70 control groups had average ages of 41.62±2.16 and 44±1.10. 95 participants had menorrhagia, which was the most common ailment in both groups. In contrast to the controls, the uterine fibroid cases had significantly higher rates of anemia (54.2%), OCP (12.8%), infertility (11.4%), and abortion (37.1%) (P<0.001). 48.5% of uterine fibroids had hypertension, compared to 17.1% of controls (P<0.001).
Conclusion: There is a considerable relationship between uterine fibroids and hypertension. Anemia, infertility, and abortion are higher in uterine fibroid cases.
DOI: 10.63475/yjm.v4i1.0005
Keywords: Hypertension, Uterine Fibroid, Factors Relationship, Case-control.
Pages: 160-163
View: 12
Download: 30
DOI URL: https://doi.org/10.63475/yjm.v4i1.0005
Publish Date: 23-05-2025
Full Text
One prevalent chronic condition is hypertension. Between 3% and 5% of pregnant women worldwide suffer from hypertensive disorders of pregnancy (HDP), which is quite prevalent. In women of reproductive age, uterine fibroids are now a risk factor for hysterectomy and a public health problem. [1] The primary cause of maternal mortality, this condition claims the lives of nearly one-third of hospitalized mothers. [2] Women with chronic hypertension are more likely to experience pregnancy-related illnesses and unfavorable pregnancy outcomes. A frequent benign tumor in women of childbearing age, uterine fibroids are linked to unfavorable pregnancy outcomes. [3] Despite being the most prevalent benign pelvic tumor in women, uterine fibroids can cause serious symptoms like anemia and excessive menstrual flow, as well as infertility and premature childbirth. [4]
Systemic impacts show that uterine fibroids are associated with higher blood pressure (BP) in women who are not pregnant. [5] Previous study research on 8,401 uterine fibroid patients found a strong correlation with hypertension. [6] In addition to the location, quantity, and size of uterine fibroids, vascular and inflammatory factors also appear to play important roles in the multifactorial relationship between uterine fibroids and hypertension. Notably, a recent study discovered that early-stage uterine fibroids may raise the risk of HDP. [7] Research is still ongoing to determine the physiological underpinnings of the relationship between uterine fibroids and hypertension. According to studies, up to 70% of women may have fibroids, but only 30% will also have clinical symptoms such as pelvic or bladder pain, infertility, pregnancy complications, irregular uterine bleeding, and abdominal pain. [8] However, the traditional diagnostic techniques for uterine fibroids include transvaginal ultrasonography and bimanual examination. [9] Smooth muscle cell modifications brought on by uterine fibroid and HTN can connect these two conditions. Therefore, the aim of this study was to assess, through a case-control design, the association between fibroids and hypertension.
Study design and setting
This case-control research was conducted from January 2023 to January 2024 at the Maternity and Children Hospital (MCH), Sakaka, Aljouf, Saudi Arabia, in the Gynecology department. There were 140 participants in all, and the study was split into two groups: the case group and the control group.
Sample size calculation
The sample size was calculated by using the following formula: N = deff u² P(1-P) / /d2, where deff is the design effect; N is the sample capacity; u is 1.96 when the confidence coefficient is 95%; and P is the probability value. According to the use of this formula, our study attains a sample size of 140.
Details regarding the case groups
Seventy patients between the ages of 20 and 50 who were admitted to this hospital for planned complete hysterectomy surgery were found to have uterine fibroids. Abdominal pain, infertility, and menorrhagia were chief complaints.
Information on the control group
At this facility, a total of 70 women aged between 20 and 50 years old were admitted for planned non-fibroid complete hysterectomy operations. The control group's symptoms, such as menorrhagia, infertility, and stomach pain, are the same as those of the case group.
Inclusion and exclusion criteria
Participants without a history of high blood pressure or those who had not checked their blood pressure in the previous two years were included. Additionally, those with a diagnosis of hypertension and those on antihypertensive medications were excluded.
Collection of data
We gathered information including demographic criteria, size and number of fibroids, history of infertility, history of taking oral contraceptive pills (OCP), thyroid disease, anemia, and diabetes. We also included information about the history of abortion, the number of abortions, the number of pregnancies, and the complaints made at the time of admission. For both groups, we have taken blood pressure readings twice a day at 30-minute intervals and recorded them. Systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg, or a patient on antihypertensive medication, are considered hypertensive.
Statistical analysis
The data were examined using the statistical tool for SPSS version 25. The results of the study were presented as mean ± standard deviation (SD) for numerical and categorical variables, or frequency (%). When the data were not normally distributed, we presented the "median and range." The comparison analysis was conducted using the chi-square test and logistic regression, and the level of significance was established at p< 0.05. The independent t-test was used to compare the two groups' mean differences in numerical variables.
Ethical considerations
The Research Ethics Committee of Jouf University, accredited by the IRB, approved research project no. 18-08-42 in Saudi Arabia.
Participants' characteristics
Our study included 140 participants in total, split into two groups (control and cases). Both cases and control groups were included; the cases group had uterine fibroids with a mean age of 40.66 and was awaiting surgery. The control group, which is awaiting non-fibroid gynecological surgery, has an average age of 43.31. All participants' characteristics and chief complaints are shown in (Table 1) and (Figure 1). Menorrhagia was common in both groups at 60% and 75.7%, respectively. Anemia (54.2%), thyroid disease (14.4%), and history of abortion (37.1%) were all substantially higher in cases than in control groups, with a significance level of P<0.001. The uterine fibroid cases had a median size range of 68.7 (12-200) mm and a median number and range of myomas of 2(2-4).
Table 1. The clinical characteristics of study cases and control cases
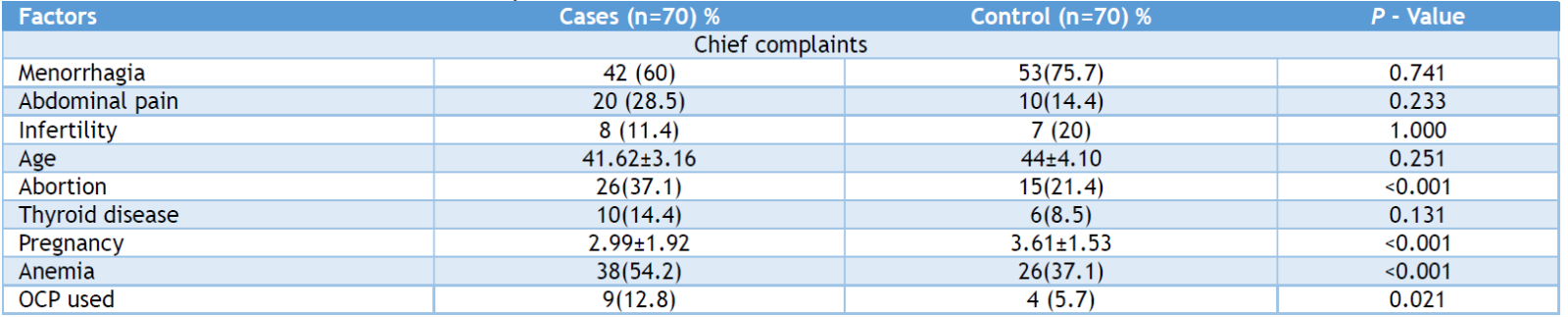
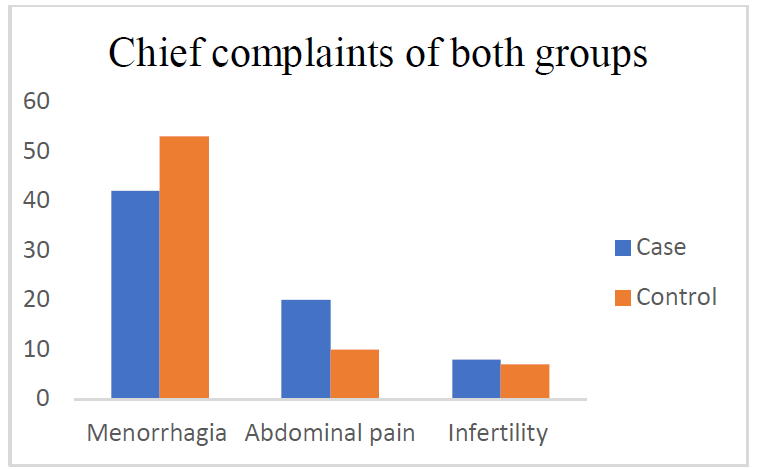
Figure 1: The chief complaints for the control and uterine fibroids groups are compared.
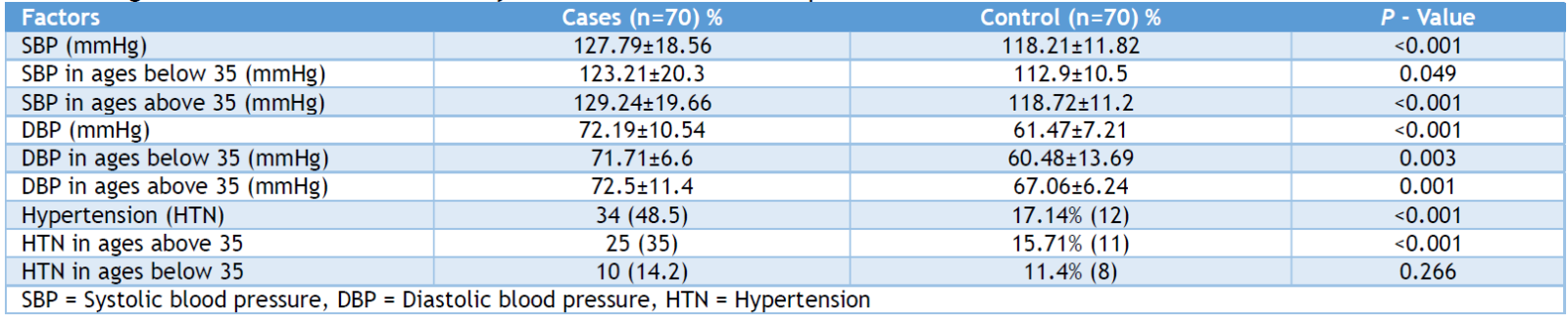
Blood pressure as a parameter in both groups
Records of blood pressure readings that were taken twice at 30-minute intervals and were identical for both groups were included. Each blood pressure measurement is shown in (Table 2). In the case and control groups, the mean SBP and DBP were 127.79±18.56, 118.21±11.82, and 72.19±10.54, 61.47±7.21, respectively (P<0.001). Uterine fibroids were shown to have significantly greater levels of hypertension (P <0.001). Ages were separated into two groups: those under 35 and those beyond 35. In cases with uterine fibroids, the SBP, DBP, and hypertension over the age of 35 were shown to be statistically significant (P <0.001).
Table 2: Age-based correlation between systolic and diastolic blood pressure in cases with uterine fibroids
Binary logistic regression
The present study determined the odds ratio obtained from the data analysis. All covariates were included in the binary logistic regression if their p-value was less than 0.05. The related factors, such as anemia, number of pregnancies, chief complaints of menorrhagia, and abdominal pain, were significantly correlated with higher SBP. (Table 3) displays all of the aforementioned data. Blood pressure and other factors such as myoma size and number, OCP intake, infertility, and abortion did not significantly correlate (p>0.05).
Table 3: Crude and adjusted p values and odds ratios.

The only significant factors in this study with uterine fibroid cases that are shown in (Table 4) were the coefficients of anemia (p=0.017) and reason for referral (chief complaint of stomach discomfort and menometrorrhagia; p=0.001). Abdominal pain, menometrorrhagia (p=0.001), and anemia (p=0.018) were the main complaints that predicted increased systolic blood pressure.
Table 4. Relationship between anemia, menorrhagia, and abdominal pain in cases of uterine fibroids(n-70).

This is the first study that we are aware of that examines the relationship between hypertension and uterine fibroids in Aljouf, Saudi Arabia. This study was created as a case and control. This study involved a total of 140 individuals who were enrolled at the Gynecological Department of the Maternity and Children Hospital (MCH) in Sakaka, Aljouf, Saudi Arabia. 140 individuals were split into two groups: 70 in the case group and 70 in the control group. Both cases—one with a uterine fibroid and one without—were scheduled for surgery at the same facility. According to our findings, there are no appreciable age differences between individuals with uterine fibroids and those without, and the condition primarily affects younger patients. The most prevalent causes of uterine fibroids are thought to be menorrhagia and abnormal uterine bleeding, with anemia also being attributed to the condition. Our study's findings were consistent with those of other studies. [11,12] According to certain research, submucosal myoma was the primary cause of anemia. [13,14] Our results showed that uterine fibroids had a significant (P<0.001) impact on pregnancy, abortion, and infertility. According to our findings, OCP use is more important in cases of uterine fibroids. Nonetheless, OCP has been shown to lessen menstruation disorders in individuals with uterine fibroids. [13] Our study's primary objective was to demonstrate the relationship between uterine fibroids and hypertension. Patients with uterine fibroids had three times the frequency of hypertension and noticeably higher systolic and diastolic blood pressures in our study. Similar findings were found in earlier research, although. [15,16] According to one concept, hypertension may have a similar effect on uterine smooth muscle fibroid growth and development as atherosclerotic alterations in artery smooth muscles. In this study, higher SBP was associated with patients who were admitted with anemia or primary complaints of abnormal uterine bleeding and abdominal pain. Patients with uterine who were older than 35 years old had the highest prevalence of hypertension.
Limitation
The primary limitation of our research is that it was conducted at a single center, which raises concerns regarding the applicability of our findings to all hospitals across the Kingdom of Saudi Arabia.
Uterine fibroid patients are known to be at risk for cardiac disease, particularly hypertension. Infertility, anemia, hypertension, and abortion were more common in uterine fibroid cases. Therefore, we advised that in cases of uterine fibroids, especially those with a history of anemia, menorrhagia, and abdominal pain, a linked study of hypertension should be required.
AUTHORS’ CONTRIBUTION
Each author has made a substantial contribution to the present work in one or more areas, including conception, study design, conduct, data collection, analysis, and interpretation. All authors have given final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
SOURCE OF FUNDING
None.
CONFLICT OF INTEREST
None.
References
- Haan YC, Diemer FS, Van der Woude L, Van Montfrans GA, Oehlers GP, Brewster LM. The risk of hypertension and cardiovascular disease in women with uterine fibroids. J Clin Hypertens (Greenwich) 2018;20(4):718-26.
- Becker ER. National trends and determinants of hospitalization costs and lengths-of-stay for uterine fibroids procedures. J Health Care Finance. 2007;33(3):1-16.
- Fields K, Neinstein L. Uterine myomas in adolescents: case reports and a review of the literature. J Pediatr Adolesc Gynecol. 1996;9(4):195-8.
- Bulun SE. Uterine fibroids. N Engl J Med. 2013; 369:1344–1355.
- Chen Y, Lin M, Guo P, Xiao J, Huang X, Xu L, et al. Uterine fibroids increase the risk of hypertensive disorders of pregnancy: a prospective cohort study. J Hypertens .2021; 39:1002–1008.
- Chen Y, Xiong N, Xiao J, Huang X, Chen R, Ye S, et al. Association of uterine fibroids with increased blood pressure: a cross-sectional study and meta-analysis. Hypertens Res. 2022; 45:715–21.
- Laughlin SK, Baird DD, Savitz DA, Herring AH, Hartmann KE. Prevalence of uterine leiomyomas in the first trimester of pregnancy: an ultrasound-screening study. Obstet Gynecol. 2009; 113:630–5.
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100-7.
- Vitiello D, McCarthy S. Diagnostic imaging of myomas. Obstet Gynecol Clin North Am. 2006;33(1):85-95.
- Sabrina Q. Rashid, Yi-Hong Chou, Chui-MeiTiu. Ultrasonography of Uterine Leiomyomas. Journal of Medical Ultrasound. 2016; 24:3-12.
- Horjus DL, Bokslag A, Hutten BA, van den Born BH, Middeldorp S, Vrijkotte TGM. Creatine kinase is associated with blood pressure during pregnancy. J Hypertens. 2019; 37:1467–1474.
- Ciebiera M, Włodarczyk M, Zgliczyn ´ska M, et al. The role of tumor necrosis factor in the biology of uterine fibroids and the related symptoms. Int J Mol Sci. 2018; 19:3869.
- Verduijn M, Siegerink B, Jager KJ, Zoccali C, Dekker FW. Mendelian randomization: use of genetics to enable causal inference in observational studies. Nephrol Dial Transplant. 2010 25:1394–8.
- Visscher PM, Brown MA, McCarthy MI, Yang J. Five years of GWAS discovery. Am J Hum Genet. 2012; 90:7–24.
- Orekoya O, Kuye-Kuku T, Fabamwo A, Akinola O, Ayanbode O. Comparative plasma levels of angiotensin II in women with or without uterine fibroid in Lagos state university teaching hospital, Ikeja, Lagos, Nigeria. J Gynecol Res Rev Rep. 2022 (4) 2022; 149:11-3
- Ziogas A, Papadopoulou A, Kalantzi S, Lamari I, Poulopoulou D, Liasidi P, et al. 321 the correlation between uterine fibroids and hypertension: a bilateral approach. Europ J Obstetr Gynecol Reprod Biol. 2022;270: e92.