Full HTML
A Comparative Study of Serum Leptin in Normotensive and Pre-eclamptic Nigerian Women
Osamudia Okhionkpamwonyi1,2, Innocent Okoacha1,2, Aimiehinor E Akhator1,2, Patrick I Okonta1,2
Author Affiliation
1 Consultant, Department of Obstetrics and Gynecology, Delta State University Teaching Hospital, Oghara, Delta State, Nigeria.
2 Honourary Consultant, Department of Obstetrics and Gynaecology, Delta State University, Abraka, Delta State, Nigeria
Abstract
Background: Pre-eclampsia remains a significant contributor to maternal and perinatal morbidity and mortality. Research into changes associated with the disease offers some hope into identifying predictive and prognostic factors. In recent times, serum leptin has attracted interest as a possible marker for the disease. The aim of this study was to determine and compare the serum leptin levels in normotensive and pre-eclamptic pregnant women attending antenatal clinic at the Delta State University Teaching Hospital, Oghara, Delta State, Nigeria.
Methods: This was a prospective case-control study design at the Delta State University Teaching Hospital, Oghara, Nigeria in which sixty three pregnant women who received antenatal care and developed pre-eclampsia were recruited into the study. For each selected pre-eclamptic, a matched normotensive was selected as control. Serum leptin level was measured by radio-immunoassay (RIA) ELISA.
Results: There was a statistically significant difference in mean serum leptin levels between the normotensive and pre-eclamptic pregnant patients 15.11±4.81 ng/dl vs 38.98±8.66 ng/dl; p<0.001. Furthermore, there was a statistically significant difference in mean leptin levels between mild and severe pre-eclampsia; 16.49±8.22 ng/dl vs 39.03±8.58 ng/dl;p<0.001.
Conclusion: This study revealed an association between serum leptin level and pre-eclampsia. Serum leptin may be a potential marker for pre-eclampsia and deserves further investigation.
DOI: 10.63475/yjm.v4i1.0002
Keywords: Pregnancy, Serum Leptin, Pre-eclampsia, Nigerian Women, DELSUTH
Pages: 123-127
View: 13
Download: 35
DOI URL: https://doi.org/10.63475/yjm.v4i1.0002
Publish Date: 22-05-2025
Full Text
Pre-eclampsia is a common complication of pregnancy associated with high maternal and perinatal morbidities and mortalities in both developed and developing countries.[1-4] In Nigeria, pre-eclampsia with eclampsia, is listed as one of the top three major causes of maternal mortality [5] Pre-eclampsia is a syndrome, defined as the onset of hypertension and proteinuria after 20 weeks of gestation in previously normotensive and non-proteinuric women. [6,7] Recently, It can also be diagnosed in the absence of proteinuria when there is evidence of maternal end-organ or uteroplacental dysfunction that is attributable to the disease condition. [7] It affects approximately 2-10% of pregnancies worldwide and in Nigeria, it ranges from 2% to 16.7% with approximately 37,000 women dying from pre-eclampsia annually. [3,8-10]Considering the significant contribution of pre-eclampsia/eclampsia to maternal and perinatal morbidity and mortality, a lot of effort has been devoted to understanding the pathophysiological basis of the disease. Although the precise mechanism of the disorder remains elusive, however, emerging consensus is that it is a complex polygenetic trait in which maternal and fetal genes as well as environmental factors are involved. [5,6,11] Recently, alterations in serum leptin have been considered as one of the pathophysiological basis underlying pre-eclampsia. [2] Leptin is a 16Kda non-glycosylated polypeptide product of the obese (Ob) gene. [2] It is mainly produced and secreted by the white adipose tissues (fat cells) in proportion to its mass. [12,13] The gene encodes 167 amino acids, located on the long arm of chromosome 7. [12,14,15] Leptin is also produced by the placenta16 and the placenta plays a role in increasing the maternal plasma leptin concentrations during pregnancy. Emerging researches show that there is also an increase in serum leptin levels in pre-eclampsia and leptin is classified as one of the maternal metabolic syndrome markers of pre-eclampsia. [6]
The relationship between pre-eclampsia and serum leptin has continued to generate considerable interest among researchers. So far, studies on serum leptin in pregnancy have been mostly from the Middle East, Europe, and North America. [10-12,16] To date there are few studies on serum leptin in pregnancy in the sub-Saharan region, Nigeria inclusive. This study aimed to determine and compare the serum leptin levels in normotensive and pre-eclamptic pregnant women attending antenatal clinics at the Delta State University Teaching Hospital, Oghara, Delta State, Nigeria.
Study design, population, and setting
This prospective case-control study was conducted at the Delta State University Teaching Hospital, Oghara, Delta State over a period of 36 months (January 1, 2016- December 31, 2018). Pregnant women who received antenatal care and developed pre-eclampsia were recruited into the study. For each selected pre-eclamptic patient, the next presenting normotensive pregnant woman matched for age, parity, gestational age, and body mass index (BMI) was selected as control.
Exclusion criteria
Women with multiple gestations, molar gestation, eclampsia and HELLP syndrome, chronic hypertension, previous history of cardiac disease, diabetes in pregnancy, gestational diabetes mellitus, HIV, renal disease, and liver disease or who were having the disease in index gestation and non-consenting patients were excluded from the study.
Sample size calculation
The desired sample size was determined using the formula for a case-control study by Charan et al [17] with a standard deviation (obtained from a previous study =13.2 The minimum sample size for each group was 63 after adjustment for 10% attrition.
Patients recruitment
The purpose and nature of the research were explained to the participants and informed consent was obtained from participants, including guardians and/or spouses of patients less than 18 years of age.
After counseling, patients who gave written consent were recruited into the study. Their blood pressure was estimated twice, 5 minutes apart (taking mean values) using a mercury sphygmomanometer desk type with an appropriate cuff in the semi-recumbent position after 5-10 minutes of rest. Their urine sample was analyzed using a dipstick urine and the result was interpreted as follows: 30mg/dl (+), 100mg/dl (2+), 300mg/dl (3+), 1000mg/dl (4+)
5mls of venous blood was drawn from the ante cubital vein from all the subjects following the application of a tourniquet under strict aseptic measures after 10 minutes of rest in a plain sterile bottle and analyzed for serum leptin. For those who developed pre-eclampsia in the second trimester and managed conservatively till the third trimester, a follow-up blood sample for leptin estimation was taken again in the third trimester. The serum leptin level was measured by radio-immunoassay (RIA) ELISA kits manufactured by GenWay Biotech Inc, San Diego, USA. The sample was collected into a microfuge bottle and analyzed immediately or stored at -20oC if analyzed within 24 hours and at -70.0 oC after 24 hours. Serum (Substrate solution) was extracted after subjecting the sample to centrifugation. The wash solution, substrate solution, leptin standard, and calibrator diluents were reconstituted as specified by the manufacturer’s instructions. The absorbance of the resulting yellow product measured spectrophotometrically at 450 nm was proportional to the concentration of leptin. A standard curve was constructed by plotting absorbance values against concentrations of Standards and concentrations of unknown samples were determined using this standard curve.
Statistical analysis
All collected data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 21. Test of statistical significance was done using the student’s t-test for continuous variables and chi-square tests for categorical variables and odd ratio calculated at 95% confidence intervals (CI). P-valve less than 0.05 (p<0.05) was considered as statistically significant.
Ethical considerations
Ethical approval was obtained from the ethical committees of the Delta State University Teaching Hospital (Reference number: DELSUTH/HREC//2014/029.
RESULTS
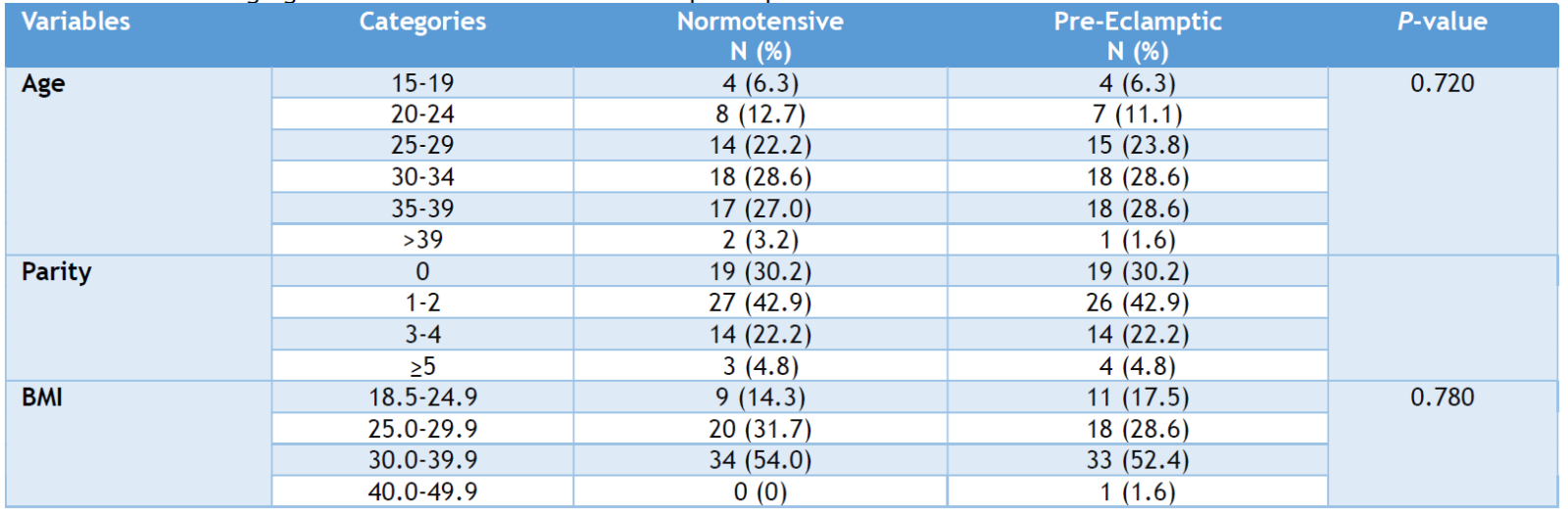
A total of 126 pregnant patients; 63 normotensive (controls) and 63 pre-eclamptic (cases), were recruited in this study. They were matched for age, gestational age, parity, and body mass index. The age range was between 15 to 39 years, with a mean age of 30.56 ± 6.01 years in the normotensive group and 30.17 ± 5.99 years in the pre-eclamptic group. This was not statistically significant (p=0.720), (table 1). The parity was between 0 to 6, with a median parity of 1 in both case and control groups. There was no difference in the mean body mass index between the two groups. 29.98 ± 4.96 kg/m2 in the control group and 30.23 ±5 .15 kg/m2 in the pre-eclamptic patients (p-value=0.780), (Table 1).
Table 1. Socio-demograghic characteristics distribution of participants
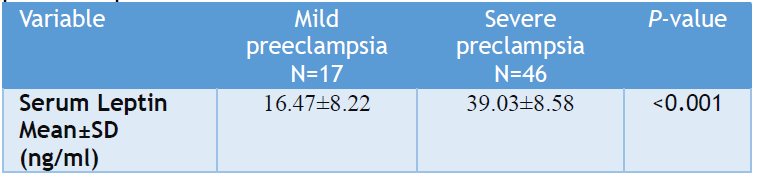
There was a marked difference in mean serum leptin levels between the two groups: normotensive and pre-eclamptic pregnant patients: 15.11 ± 4.81 ng/dl as compared to 38.98 ±8.67 ng/dl (OR=16.6, p<0.001, 95% CI:12.9-36.8)(Table 2). Among the pre-eclamptic patients, there was a difference in mean leptin levels according to the severity of pre-eclampsia. 16.49 ± 8.22 ng/dl in mild pre-eclamptic group and 39.03 ± 8.58 ng/dl in severe pre-eclamptic group (Table 3). This was statistically significant (OR=6.7; 95% CI=2.8-13.7, p<0.001).
Table 2. Mean serum leptin levels in normal pregnant women (controls) and in pre-eclamptic women
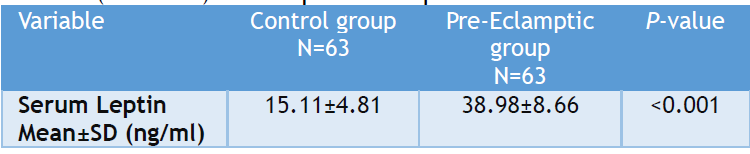
Table 3: Mean serum leptin levels according to the severity of preeclampsia
Three pre-eclamptic had the diagnosis made in the second trimester with a mean serum leptin level of 10.52 ± 2.07 ng/dl while the remaining sixty pre-eclamptic patients with mean serum leptin of 38.52 ± 4.63 ng/dl were made in third trimester. The corresponding values in normotensive controls were 7.24 ± 3.11ng/dl and 11.27 ± 3.84 ng/dl respectively. The three patients who were managed conservatively to the third trimester (mean gestational age of 30.2 ± 1.6 weeks) had their mean serum leptin levels increased from 10.52 ± 2.07 ng/dl to 35.78 ± 2.16 ng/dl. This was statistically significant (OR=4.0,95%CI=8.1-12.8, p<0.001) (Table 4). There was a statistical increase in serum leptin levels for both normotensive and pre-eclamptic patients whose BMI was greater than 30kg/m2 (Table 5).
Table 4. Serial serum leptin levels in women who developed pre-eclampsia in second trimesters and followed-up to third trimester
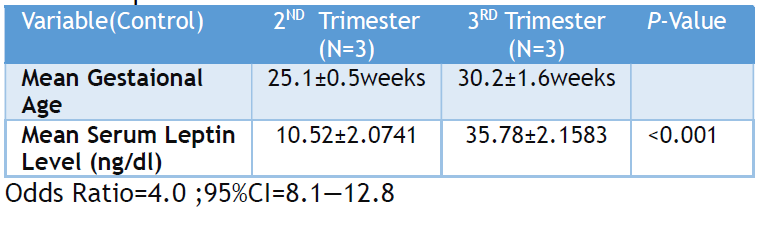
Table 5: Association between body mass index and serum leptin levels

This study was conducted to determine the serum leptin levels in normotensive and pre-eclamptic pregnant women and to compare the relationship between serum leptin levels and its severity in pre-eclampsia, a disease of many theories and significant contributor to maternal morbidity and mortality, especially in the third world countries.
This study revealed that serum leptin levels in pre-eclamptic women were significantly elevated, compared to matched normotensive woman (38.98 ± 8.67 ng/dl vs 15.11 ± 4.81 ng/dl; OR=16.6, p<0.001, 95%CI:12.9-36.8). Our finding coincides with reports by UzmaIftikhar et al, Acromite et al, De-Knegtet al, Firdous et al, and EL Shahat et al. [2,6,18-20] Placental leptin expression and placental leptin proteins increased in pre-eclampsia and correlate with circulating levels. [18,21] In pre-eclampsia, placental ischemia/hypoxia triggers the cascade of events that ultimately results in the maternal manifestations of the disease which is responsible for the increase in leptin level and increase in inflammatory mediators and cytokines produced by monocyte/ macrophage. [19,22-24] The higher concentrations of serum leptin in pregnancies complicated by pre-eclampsia are consistent with observations that placental expression of leptin mRNA is up-regulated in pre-eclamptic placentae [18], and leptin receptors trigger a noradrenaline turnover within the brown adipose tissue so that sympathetic activity is increased in the feto-maternal unit, stimulating fetal wastage and sudden intrauterine demise. [25] In contrast to our findings, some authors did not find any increase in serum leptin in pre-eclamptics. [26] Thomas Lami et al found that mean serum leptin levels were lower in pre-eclamptic patients27 while Martinez-Abundis et al found unchanged circulating serum leptin levels in pre-eclamptics. [28]
Our study demonstrated an association between serum leptin levels and severity of pre-eclampsia, the serum leptin levels were statistically higher in the severe group than in the mild group (39.03 ± 8.58 ng/dl vs 16.49 ± 8.22 ng/dl OR=6.7, 95%CI=2.8-13.7, p<0.001). Our finding is similar to earlier reports by UzmaIftikhar and Salimiet et al., [2,29] impaired renal function is a pathophysiological component of severe pre-eclampsia and the elevated levels of serum leptin concentrations may reflect reduced renal clearance. Also, higher serum leptin levels in severe pre-eclampsia may be due to possible haemo-concentration caused by the association of pre-eclampsia with reduced plasma volume. [30] More so, the exaggerated placental ischemia in severe pre-eclampsia may also explain the rapid increase in serum leptin levels concentrations during the late third trimester and in severe pre-eclampsia as placental hypo perfusion produces local hypoxia which consequently augments leptin gene expression in the placenta. [31]
The fact that preeclampsia is a progressive disease is reflected in the increase in serum leptin levels of pre-eclamptic diagnosed in the second trimester and followed up to the third trimester. This finding is in line with earlier reports by Salimi and Masuyama et al. [29,32] The study also demonstrated an association between serum leptin levels and body mass index, the serum leptin levels were statistically higher in patients with higher body mass index, (P<0.001). This is similar to the report by Agbogu-Ike et al. [33]
Limitations
Although the study period (2016–2018) may be considered outdated, it still highlights the issue of elevated leptin levels in women with pre-eclampsia. The methodology used in this study could not conclude if the significant difference in serum leptin levels is a cause or consequence of pre-eclampsia. Hence, further studies will be required to demonstrate this significant difference in serum leptin levels in our women (cohort study involving serial blood samples throughout pregnancy starting from the first trimester).
This study has shown that there is a marked increase in serum leptin level in pre-eclampsia compared to normotensives and there is also an association between serum leptin and the severity of pre-eclampsia among pregnant women in Nigeria. However, whether this association is causal or casual would need to be determined by further studies.
ACKNOWLEDGEMENT
A special appreciation to all resident doctors and nurses of the department of Obstetrics and Gynaecology for their efforts and commitment during the study and Mr Harlims Oformola for his laboratory supervision and analysis.
AUTHORS’ CONTRIBUTION
Each author has made a substantial contribution to the present work in one or more areas including conception, study design, conduct, data collection, analysis, and interpretation. All authors have given final approval of the version to be published, agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
SOURCE OF FUNDING
None.
CONFLICT OF INTEREST
None.
References
- Njelita IA, Nwachukwu CC, Eyisi GI, Akabuike JC, Ezenyeaku CA, Ifeadike CO. Determinants of Preeclampsia in a Tertiary Hospital in South East Nigeria, Intl J Med Sci. 2021; 8(6):5490-5497
- Uzma Iftikhar A, Mehjabeen AI, Khemomal AK. Evaluation of serum leptin levels during normal pregnancy and preeclampsia. J Ayub Med Coll Abbottabad. 2008;20(4):137-140.
- Okoye HC, Efobi CC, Ugwu EO, Nwagha TU. ABO Blood Group as a Biomarker of Preeclampsia among Antenatal Clinic Attendees in Nigeria. Niger J Clin Pract. 2020;23(5):729-733.
- Adeyeye OV, Ebubechukwu NV, Olanrewaju OF, Eniayewun AG, Nwata C, Effiong FB,Unim B. Management and Prevention of Pre-Eclampsiain Nigeria. Healthcare. 2023;11(13): 1832
- Ekele BA, Airede LR, Legbo JN, Yabubu A Nnadi DC, Gana MA.Spontanous liver rupture in preeclampsia.Afri J Med Sci. 2006;35(1):103-105.
- Acromite M, Ziotopoulu M, Orlova C, Mantzoros C. Increases leptin levels in preeclampsia: Association with BMI, estrogen and SHBG levels. Hormone. 2010;3(1):46-62.
- ACOG. Clinical Management Guidelines for Obstetrician – Gynecologists. Obstet Gynecol.2019;133(76):168–86.
- Uzan J, Carbonne M, Piconne O, Asmar R, Jean-Marc A. Preeclampsia: pathophysiology, diagnosis and management. Vasc Health Risk Manag.2011;7:467-474.
- Thapa K, Jha R. Magnesium sulphate: a life saving drug. JNMA J Nepal Med Assoc. 2008;47:104-108.
- Olaoye T, OyerindeOO,Elebuji OJ, Ologun O. Knowledge, Perception and Management of Pre-eclampsia among Health Care Providers in a Maternity Hospital. Int J MCH AIDS 2019;8(2):80-88.
- Jerath R, Barnes VA, Fedel HE. Mechanism of development of preeclampsia linking breathing disorder to endothelial dysfunction. Med Hypotheses. 2009;73(2):163-166.
- Martinez-Sanchaz N, There and Back Again: Leptin Actions in the White Adipose Tissue. Int J Mol Sci, 2020;21(17):6039.
- Tal R. The role of hypoxia and hypoxic inducible factor-1 alpha in preeclampsia pathogenesis. BiolReprod. 2012;87(6):134-139.
- Szpera-Gozdziewicz A, Breborowicz GH. Endothelial dysfunction in the pathogenesis of preeclampsia. Front Bio Sci.2014;19:734-746.
- Myatt L, Clifton RG, Robert JM, Spong CY, Hauth JC, Varner MW et al. First trimester prediction of preeclampsia in nulliparapous women at low risk. Obstet Gynecol. 2012;119(6):1234-1242.
- Ghojazaeh M, Amami-Aghdash S, Mohammadi M, Vosoogh S. Prognosis and risk factor for early diagnosing of preeclampsia in nullipara. Niger Med J.2013;54(5):344-348.
- Charan J, Biswas T. How to calculate sample size for different study designs in medical research. Indian J Psychol Med. 2013;35:121-126.
- De-Knegt VE, Hedley PL, Kanters JK, Thagaard IN, Krebs L, Christiansen M, Lausten-Thomas U.The Role of Leptin in Fetal Growth during Pre-Eclampsia. Int J Mol Sci. 2021;22(9): 4569. doi/10. 3390/ijms22094569Mol Hum Reprod. 2006; 12:551-556.
- Firdous M, Abdul RM, Sajida Y, Tahir SM. Role of serum leptin level as a marker of severity of preeclampsia. J Ayub Med Coll Abbottabad. 2008;20(1):13-15.
- Shahat EL, Mohamed A, Ahmed AB, Mohamed HS, Ahmed MR . Maternal serum leptin as a marker of preeclampsia. Arch Gynecol Obstet.2013;288(6):1317-1321.
- Zeng S, Liu Y, Fan P, Yang L, Liu X. Role of leptin in the pathophysiology of preeclampsia. Placenta. 2023;142:128-134.
- De Arruda Veiga EC, Korkes HA, Salomao KB, Cavalli RC. Association of Leptin and other inflammatory markers with pre-eclampsia: A systematic review. Front Pharmacol2022;13:96600.
- Min-Jung P, Dong-Hyung L, Bo-Sun J, Young-Joo L, Jong-Kil J,Beum-Soo A, Seung-Chul K, Kyu-Sup L. Leptin, leptin receptors and hypoxia-induced factor-1a expression in the placental bedof patients with and without preeclampsiaduring pregnancy. Mol Med Reports 2018; 5292-5299.
- Wang S, Qlao FY, Feng I. High leptin level and leptin receptor Lys656Asn variant are risk factors for preeclampsia. Genet Mol Res.2013;12(3):2416-2422.
- Sucak A, Kanat-Pektas M, Gungor T, Mollamahmutoglu L. Leptin levels and antihypertensive treatment in preeclampsia. Singapore Med J. 2010,51(1):30-43.
- Asnafi N, Sharbatdaran M, Hajian K.Comparism of maternal and neonatal serum leptin levels in preeclampsia and normal pregnancy. Iran J Reprod Med.2011; 9(2):131-134.
- Thomas L, Ashworth CJ, Hoggard N, Mercer JG, Wallace JM, Lea RG. Decreased maternal serum leptin in pregnancies complicated by preeclampsia. Reprod Sci. 2001;8(2):89-92.
- Martinez-Abundis E, Gonzalez-Ortiz M, Pascoe-Gonzalez S. Serum leptin levels severity of pre-eclampsia. Arch Gynae Obstet. 2000;264(2):71-73.
- Salimi S, Farajian-Mashhadi F, Naghavi A, Mokhtari M, Shahrakipour M, Saravani M, et al. Different profile of serum leptin between early onset and late onset preeclampsia. Dis Markers. 2014;2014:628476.
- Rivera MY, Ning Y, Fredrec N. Leptin, Soluble leptin receptor and leptin gene polymorphism in relation to pre-eclampsia risk. Physiol Res. 2005; 54: 167-74.
- Bakrania BA, Spradley FT, Drummond HA, LaMarca B, Ryan MJ, Granger JP. Preeclampsia: Linking Placental Ischaemia with Maternal Endothelial and Vascular Dysfunction. ComprPhysiol 2020; 11(1):1315-1349
- Masuyama H, Segawa T, Sumida Y. Different profile of circulating angiogenic factors and adipocytokines between early and late-onset pre-eclampsia. BJOG. 2010;117(3):314-320.
- Agbogu-Ike OU, Ogoina D, Onyemelukwe GC. Leptin Concentrations in Non –Obese and Obese Non-Diabetes Nigerian Africans. Diabetes Metab Syndr Obes. 2021;21(14):4889-4902.