Full HTML
Primary mediastinal large b-cell non-hodgkin’s Lymphoma
Muad Fahmi Yousef1, Abdo Qaid Lutf2
Author Affiliation
1 Department of Medical Radiology, University of Doha for Science and Technology, Doha, Qatar
2 Deprtment of Medicine, Rheumatology Division Alkhor Hospital, Alkhor, Qatar
Abstract
No abstract
DOI: 10.18231/j.yjom.2024.032
Pages: 269-270
View: 12
Download: 18
DOI URL: http://doi.org/10.18231/j.yjom.2024.032
Publish Date: 15-12-2024
Full Text
A 23-year-old male patient with no prior chronic illness presented to the emergency department with chest pain, shortness of breath, and dry cough for two weeks. He denied fever, weight loss, night sweats, cigarette smoking, or contact with sick people. Clinical examination was unremarkable. Chest X-ray showed a wide mediastinum (Figure 1), while contrast-enhanced chest computed tomography (CT) showed a large soft tissue mass in the anterior mediastinum, which significantly displaced the visceral structures posteriorly (Figure 2). The differential diagnoses included: lymphoma, germ cell tumor, thymic carcinoma, primary sarcoma, and metastatic choriocarcinoma. A thoracic surgeon was consulted, who decided to remove the mass and send samples for histopathological examination. After histopathological examination of the removed tumor, the diagnosis of primary mediastinal B-cell non-Hodgkin lymphoma (NHL) was made. The patient was referred to a hematology hospital to continue management.
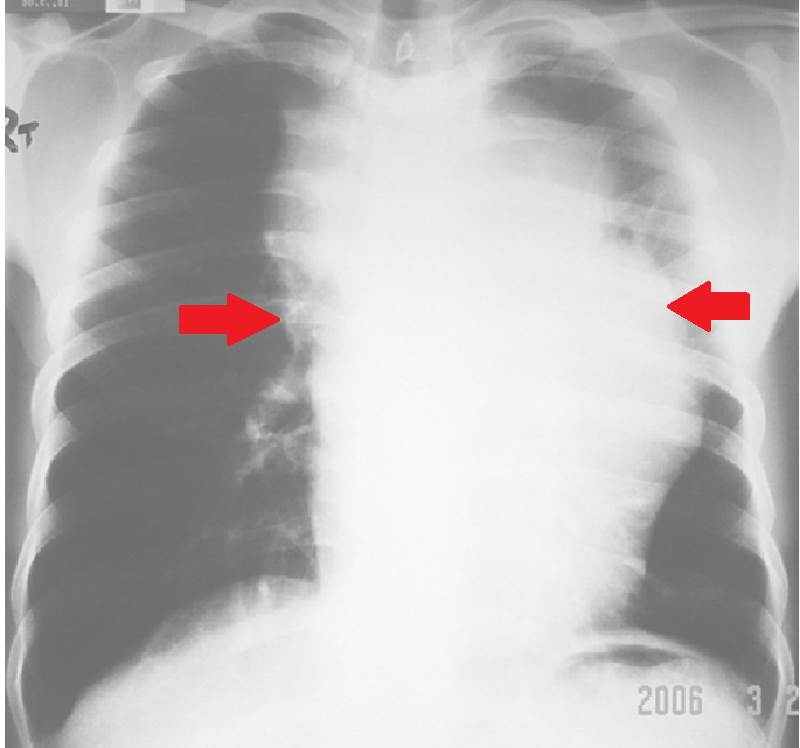
Figure 1. shows a wide mediastinum (Red arrows)
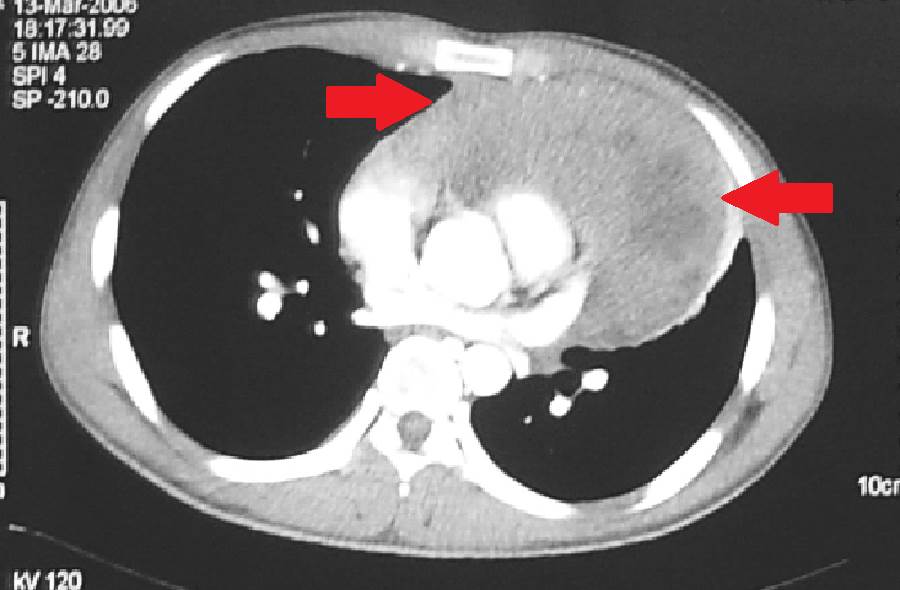
Figure 2. Shows a large soft tissue mass in the anterior mediastinum (Red arrows)
NHL is a type of neoplasm that arises from lymphoid tissues, specifically from B cell precursors, mature B cells, T cell precursors, and mature T cells (1). Primary mediastinal B-cell lymphoma represents a rare variant of NHL, comprising approximately 2-3% of all NHL diagnoses (2-4)). It occurs more frequently in female patients (4). The clinical manifestation of NHL can vary significantly; however, it is typically associated with a rapidly growing mass in the mediastinum. This mass exerts pressure on neighboring structures within the mediastinum, including the lungs, superior vena cava, and other vascular components.
The approach to managing non-Hodgkin lymphoma differs significantly depending on the particular subtype and stage of the disease. Common treatment modalities often encompass chemoimmunotherapy, radiotherapy, hematopoietic stem cell transplantation, and chimeric antigen receptor (CAR)-T cell therapy (1).
Learning points:
- Although uncommon, primary mediastinal large B-cell NHL can affect male patients.
- Despite its rarity, healthcare professionals should remain vigilant for primary mediastinal large B-cell NHL in patients who exhibit shortness of breath accompanied by a significant anterior mediastinal mass.
Consent
Written informed consent was obtained from the patient for publication of this case report.
Authors’ contribution
All authors contributed to the completion of this work. The final manuscript was read and approved by all authors.
Conflict of Interest
None.
Source of Funding
None.
References
1. Radiopaedia. Available from: https://radiopaedia.org/articles/nonhodgkin-lymphoma.
2. Mizuno R, Fujimoto S, Okamoto Y. Mediastinal huge non-Hodgkin’s lymphoma causing compression of the main pulmonary artery trunk. BMJ Case Rep. 2012;2012:2012006530.
3. Castro E. Primary mediastinal B cell non-hodgkin’s lymphoma presenting as superior vena cava syndrome and pericardial effusion in tamponade in a 28-year-old female: a case report. Chest. 2020;158(4):1448.
4. Phan AT, Randhawa JS, Johnston B, Khosravi C, Malkoc A, Arabian. Primary Mediastinal B-Cell Lymphoma Presenting as Cardiac Tamponade. J Med Cases. 2023;14(8):277–81.