Full HTML
Esophageal granular cell tumor
Yong-Xin Yang1,2,3, Wei Liu1,2,3
Author Affiliation
1Professor, Department of Medicine, The First College of Clinical Medical Science,
2Gastroenterologist, Department of Gastroenterology, Institute of Digestive Disease, China Three Gorges University,
3Gastroenterologist, Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
Abstract
A 45-year-old asymptomatic woman presented for a routine health checkup. The patient denied gastrointestinal symptoms, unintentional weight loss, and a family history of gastrointestinal malignancy. Clinical examination was unremarkable. All laboratory tests were within normal limits.
DOI: 10.63475/yjm.v3i1.4466
Pages: 64-65
View: 10
Download: 18
DOI URL: http://dx.doi.org/10.63475/yjm.v3i1.4466
Publish Date: 11-05-2024
Full Text
A 45-year-old asymptomatic woman presented for a routine health checkup. The patient denied gastrointestinal symptoms, unintentional weight loss, and a family history of gastrointestinal malignancy. Clinical examination was unremarkable. All laboratory tests were within normal limits. Upper gastrointestinal endoscopy showed a yellow-grayish, intramural, submucosal nodule of about 8×10 mm in the distal esophagus (Fig. 1a and b). The initial biopsy did not provide a clear diagnosis. Endoscopic ultrasound showed a homogenous, well-circumscribed, hypoechogenic tumor 6 mm in diameter with a sharp border and a normal mucosa extending from the submucosal layer (Fig. 1c). Histopathologic examination confirmed subepithelial, sheet-like cell formations with intersections of smooth muscles (Fig. 1d). Immunohistochemical examination identified granular cell tumor with positivity for S100 (Fig. 1e) and SOX10 (Fig. 1f). The final diagnosis of a granular cell tumor was made. Granular cell tumors are rarely located in the esophagus. Most esophageal granular cell tumors rarely cause dysphagia and chest pain, which are commonly identified as painless masses by incidental findings on endoscopy [1-3]. After a well-informed discussion of options for interventions with her, she decided to have the tumor removed. Endoscopic snare resection was performed without complications after submucosal injection.
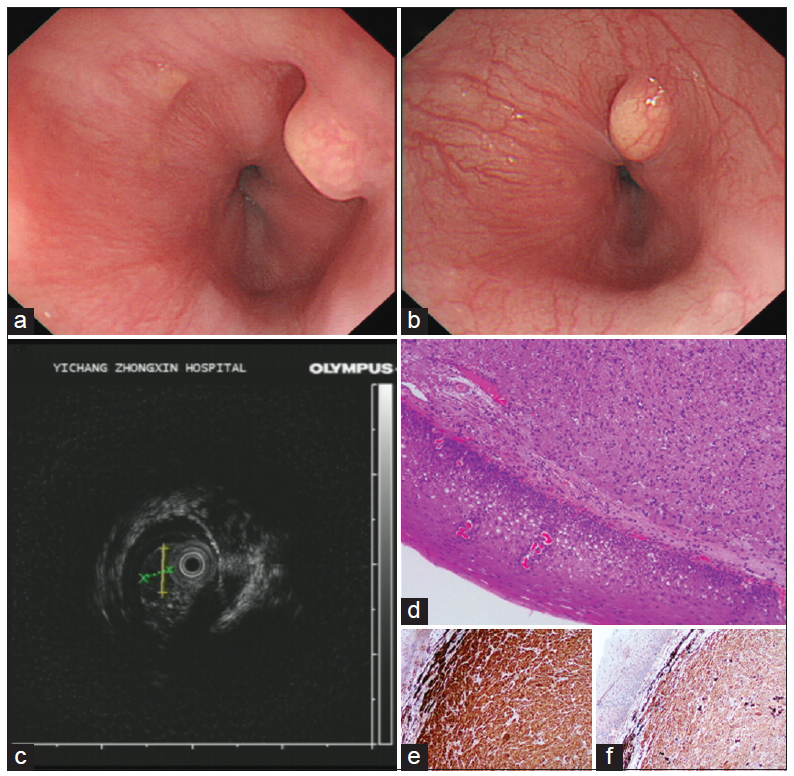
Figure 1: (a and b) Upper gastrointestinal endoscopy showed a yellow-grayish, intramural, submucosal nodule of about 8×10 mm in the distal esophagus. (c) Endoscopic ultrasound showed a homogenous, well-circumscribed, hypoechogenic tumor 6 mm in diameter with a sharp border and a normal mucosa extending from the submucosal layer. (d) Histopathologic examination confirmed subepithelial, sheet-like cell formations with intersections of smooth muscles. Immunohistochemical examination identified granular cell tumor with positivity for S100 (e) and SOX10. (f)
LEARNING POINTS
1. Gastroenterologists should bear in mind esophageal granular cell tumor whenever having a submucosal nodule.
2. Esophageal granular cell tumor may mimic leiomyoma in endoscopic findings.
3. Histopathological examination should be the first modality of investigation.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for the publication of this case report and all associated images.
AUTHORS’ CONTRIBUTIONS
All authors contributed to the completion of this work. The final manuscript was read and approved by all authors.
References
1. Revia RA, Shah R, Mandalia A, et al. Esophageal granular cell tumor: An uncommon cause of dysphagia. Cureus 2023;15:e41846
2. Ofori E, Ramai D, Lui YX, et al. Esophageal granular cell tumor: A case and review of the literature. Gastroenterol Res 2017;10: 372-5.
3. Nakajima M, Kato H, Muroi H, et al. Esophageal granular cell tumor successfully resected by endoscopic submucosal dissection. Esophagus 2011;8:203-7.